
Cardiac Cath Lab Activation for Subtle Acute Inferior STEMI
EMS responds to a 78 year old male complaining of chest pain. On initial observation the patient is pale, cool, and diaphoretic. He says to the treating paramedic, “I think I’m having a heart attack.” He states that he was watching TV when he felt a crushing pain that radiated to his arm and jaw.
Pertinent Medical History
- CABG X 2
- Stents
- CVA
- Hernia Repair
Vital Signs
- RR: 17
- HR: 75
- NIBP: 146/80
- SpO2: 98% on room air
The following 12 Lead was acquired.
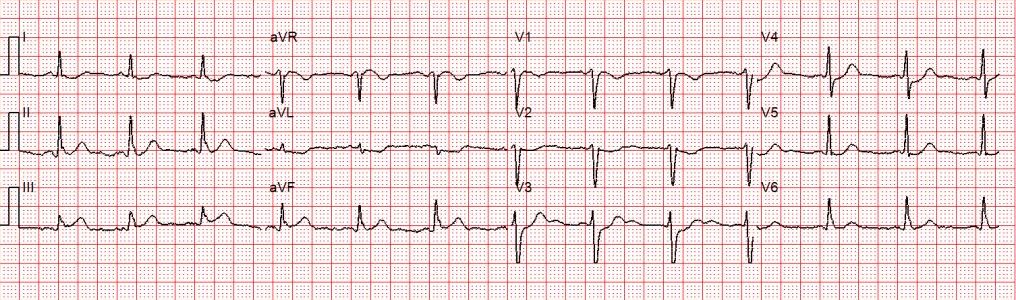
Sinus rhythm with ST depression in leads I, aVL, V2-V4, and 1mm of elevation in lead III.
Is this ECG diagnostic for an acute STEMI?
The Guidelines require new ST-segment elevation, measured at the J-point in at least 2 contiguous leads of ≥ 2 mm (men) or ≥ 1.5 mm (women) in leads V2-V3 and/or ≥ 1 mm in other contiguous leads or the limb leads.
Using this criteria, the EKG is only about 45% sensitive for an acute MI. That means that if we strictly went by mm criteria only 45 out of every 100 patients experiencing acute STEMI would be picked up on the 12-lead ECG. That’s a lot of missed occlusions.
Conversely, many patients have ST-segment elevation at baseline that is not the result of acute coronary occlusion.
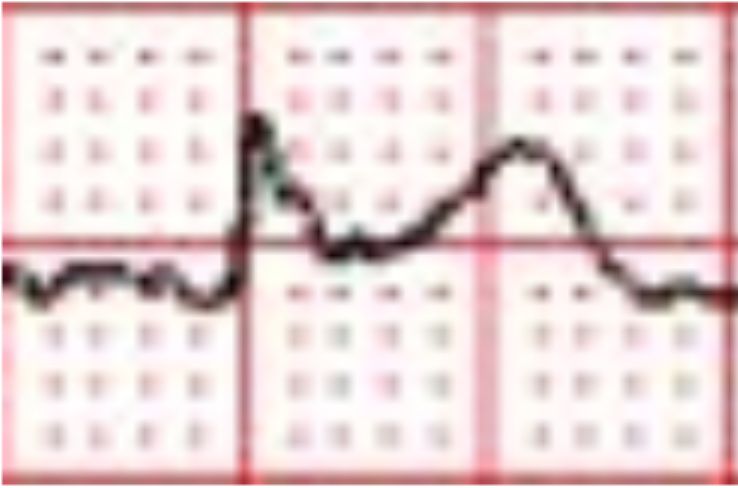
In this case lead III is the only lead that if blown up may have about 1 mm of ST-segment elevation.
According to the treating paramedic, the patient presented with classic signs and symptoms. It may be important to note that this was an experienced paramedic and his gut told him the patient was experiencing a heart attack, so he activated the cardiac cath lab.
There were no observable changes on serial prehospital 12-lead ECGs. However, there was a difference noted on the 12-lead ECG obtained on arrival in the Emergency Department.
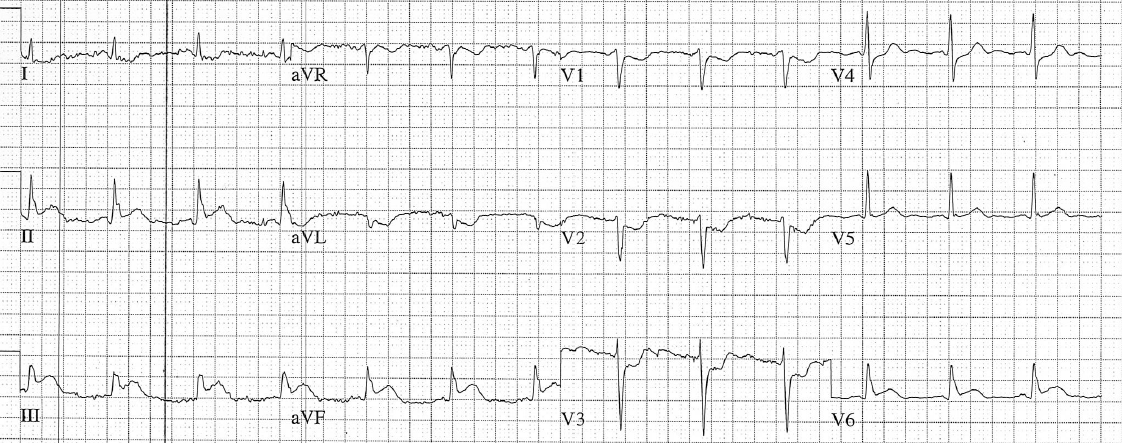
There is worsening of ST-segment elevation in the inferior leads, new ST-segment elevation in lead V6, and the reciprocal ST-segment depression in leads V1-V3 now looks diagnostic for posterior extension.
When I showed the initial ECG to other providers, most were quick to point out that the ECG was “not diagnostic” because of the absence of ST-segment elevation in 2 contiguous leads.
This is not surprising. Most ECG courses spend a lot of time going over “slam dunk” ECGs with significant ST-segment elevation so that students don’t learn to appreciate subtle signs of acute STEMI.
Looking at the first ECG we can be almost certain that the patient is experiencing acute inferior STEMI even though it does not meet millimeter criteria.
The ST-segment depression must be explained. One of the most salient points that impacted my understanding of subtle occlusions is that ischemia does not localize.
We have all been taught that subendocardial ischemia presents as ST-segment depression whereas transmural (epicardial) ischemia from coronary occlusion typically manifests as ST-segment elevation.
Subendocardial ischemia typically presents with ST-segment elevation in lead aVR with widespread ST-segment depression that does not “localize” to a particular set of leads.
In this case there is isolated ST-segment depression in the high lateral leads (I and aVL) and in the anterior leads (V1-V4).
This means that the most probable explanation for the ST-segment depression is not ischemia, but reciprocal changes from an inferior-posterior STEMI!
Always consider the possibility that a subtle STEMI is present when there is isolated ST-segment depression on the 12-lead ECG.
ST-segment depression in lead aVL is highly sensitive for acute inferior STEMI. If there is ST-segment depression in lead aVL you should consider the possibility of acute inferior STEMI, especially if there is ST-segment elevation in lead III.
ST-segment depression in lead aVL can precede ST-segment elevation in the inferior leads!
However, ST-segment depression in lead aVL can also be caused by so-called “secondary” ST/T-wave abnormalities. However, we can easily rule those out in this case because:
- The QRS is not wide – There’s no bundle branch block or WPW pattern
- There’s no high voltage – Left ventricular hypertrophy is not present
- The QRS/T angle is not “wide” – Normally in the presence of a secondary ST/T-wave abnormality there is a general pattern of T-wave discordance. That means that when the majority of the QRS complex is positive the T-wave should be negative. When the majority of the QRS complex is negative, the T-wave should be positive.
Therefore the ST-segment changes in the initial ECG should be considered primary — due to acute STEMI.
Left ventricular hypertrophy is the most common of STEMI mimics, so it may be worthwhile to review the criteria here.
What about activating the cardiac cath lab for subtle STEMIs?
Cardiac cath lab activation should be reserved for clear-cut STEMI.
Most prehospital protocols require some combination of millimeter criteria, reciprocal changes, computerized interpretation, or ECG transmission.
With appropriate education, training, and feedback, decision rules can be created to catch more subtle STEMIs but it requires buy-in from Emergency Medicine and Cardiology.
Whether there is prehospital cardiac cath lab activation or not it makes sense to transport these patients to PCI-capable hospital if possible.
STEMI is a dynamic process. If subtle changes are present, serial ECGs often reveal dynamic changes that will then prompt cardiac cath lab activation.
Case Conclusion
After the ECG was obtained in the Emergency Department the patient was taken to the cardiac cath lab. The patient suffered ventricular fibrillation and required defibrillation. He was found to have an occluded vein graft from previous bypass. The patient was re-perfused and is now doing fine.
References
Smith, Stephen. “ST-depression limited to inferior leads is reciprocal to high lateral wall and represents STEMI” Dr. Smith’s ECG Blog. Web. 14 Jan 2009
Bouthillet, Tom. “Ischemia Does Not Localize! What Does It Mean? – ECG Medical Training.” ECG Medical Training. N.p., 18 Jan. 2016. Web. 03 Feb. 2016.
Mckenna, Kim D., Elliot Carhart, Daniel Bercher, Andrew Spain, John Todaro, and Joann Freel. “Simulation Use in Paramedic Education Research (SUPER): A Descriptive Study.” Prehospital Emergency Care 19.3 (2015): 432-40. Web.
“What’s the Point of ST Elevation?” — Carley Et Al. 19 (2): 126. N.p., n.d. Web. 03 Feb. 2016. “Which Patient Should Get Acute Cath Lab Activation in MI?” EMCrit. N.p., 29 Mar. 2015. Web. 03 Feb. 2016.


Comments