EMS was dispatched to an 82-year-old female complaining of smoke inhalation following a fire originating in her clothes dryer.
On arrival at scene the patient is conscious, alert, and anxious. She is being treated with high flow oxygen in the cabin of a fire engine. She has visible soot on her clothes, hands and face.
Soot is also noted in both nostrils. Although the patient complains of a sore throat no burns are noted and the airway is patent. There is no stridor, hoarseness, or swelling. There is no problem with air entry, no cyanosis, and no use of accessory muscles.
Vital signs are assessed.
- RR: 20
- HR: 111
- NIBP: 117/70
- Temp: 37.1C / 98.8F
- SpO2: 98% with oxygen
- GCS: 15
It should be noted that pulse oximetry is unreliable for CO exposed patients.
Breath sounds are clear bilaterally.
Upon further questioning the patient admits to 5/10 non-radiating central chest pain described as “discomfort.” There is no associated diaphoresis, paleness, or nausea.
The cardiac monitor is attached.
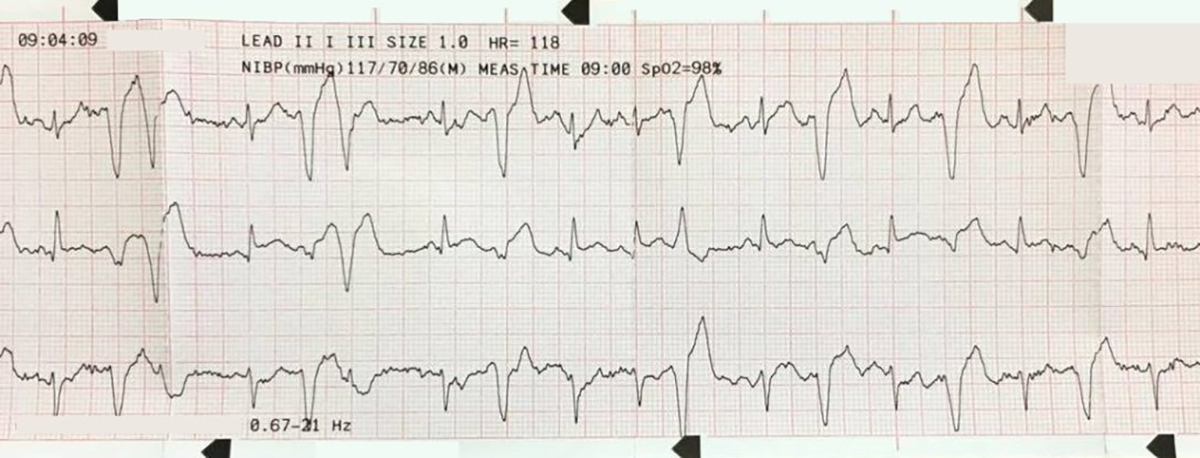
Sinus tachycardia with ventricular bigeminy
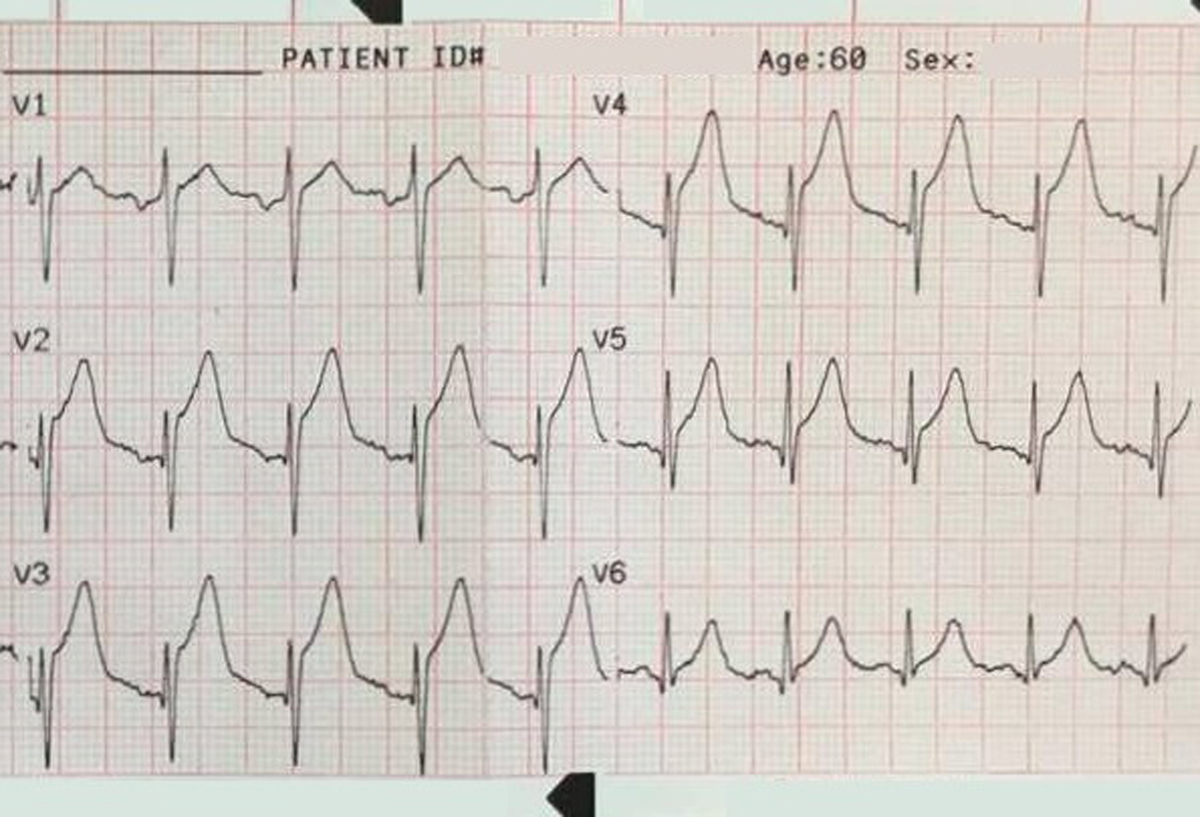
A 12-lead ECG is obtained.
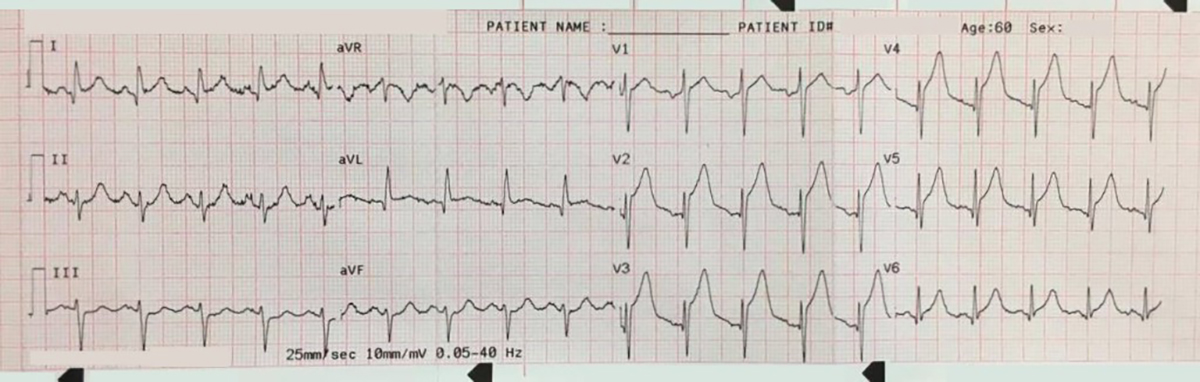
ST-segment elevation is noted in leads V1-V6 and leads I and aVL with reciprocal ST-segment depression in leads III and aVF
The 12-lead ECG was deemed to show acute anterior STEMI consistent with LAD occlusion. Pre-alert was made to the primary percutaneous coronary intervention (PPCI) center.
Treatment
ACS medication: (local guidelines)
- GTN 400 mcg sublingual spray
- Aspirin 300 mg oral
- Clopidogrel 600 mg
- Continued oxygen therapy for caution of CO levels (not routinely administered for STEMI patients)
- Patient refused any analgesia
On arrival at PPCI center
The cardiologist agreed with the ECG interpretation and the patient was taken for emergency coronary angiogram.
PPCI findings
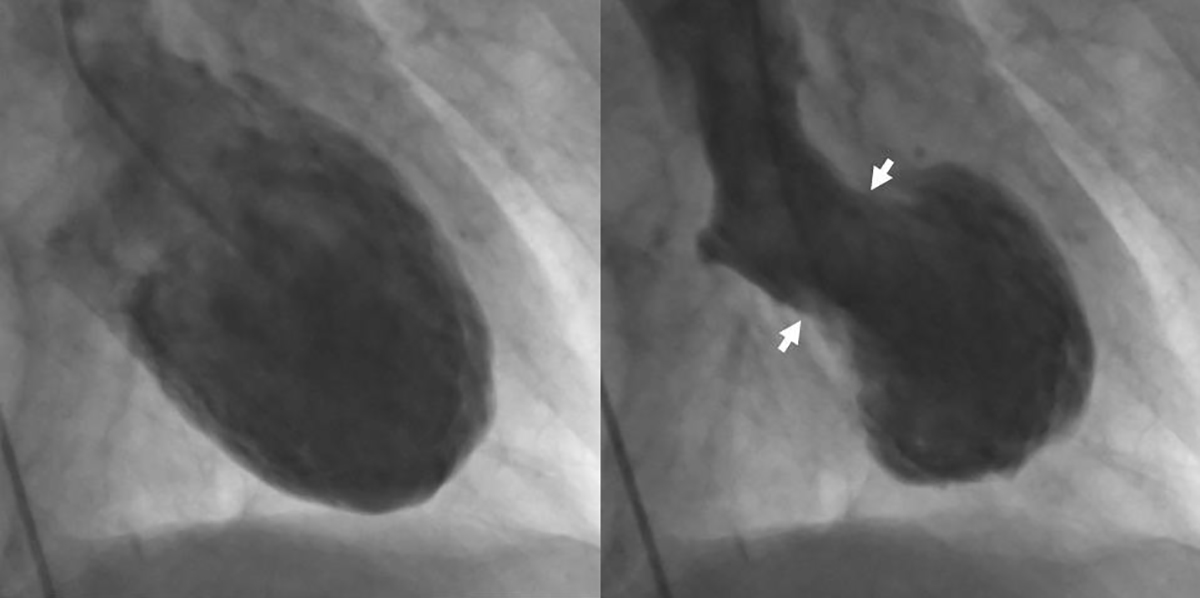
The patient displayed normal coronary arteries on angiography with no blockages but was diagnosed with takotsubo cardiomyopathy (TCM).
Takotsubo cardiomyopathy
Takotsubo cardiomyopathy is a transient cardiac condition that involves left ventricular apical akinesis (or ballooning) that can mimic acute ST-elevation myocardial infarction (STEMI). Because it is typically associated with significant emotional distress it is sometimes referred to as “broken heart syndrome” or “stress cardiomyopathy”.
The Japanese cardiologist who first described takotsubo cardiomyopathy in 1990 noticed that the left ventriculogram took on the shape of a fishing pot used to trap octopus. In Japanese name for “octopus pot” is “tako tsubo.”

EMS12Lead.com with permission
Patients with TCM typically present with chest pain and shortness of breath and ST-segment elevation on the 12-lead ECG. This can be accompanied by a rise and fall of cardiac biomarkers consistent with acute myocardial infarction. As seen in the above case, no acute thrombotic lesions are noted with angiography. Diagnostically, apical ballooning of the left ventricle is present.
Ninety percent of patients on the International Takotsubo Registry are female and have an age range of 58-75. Research suspects that this may be due to a reduction in estrogen following the menopause.
Research suggests that at least 6% of women assessed for an acute myocardial infarction present with TCM. However it is also believed that TCM is under-recognized and under-reported. The prognosis is generally excellent with a 4-8 week recovery time.
Conclusion
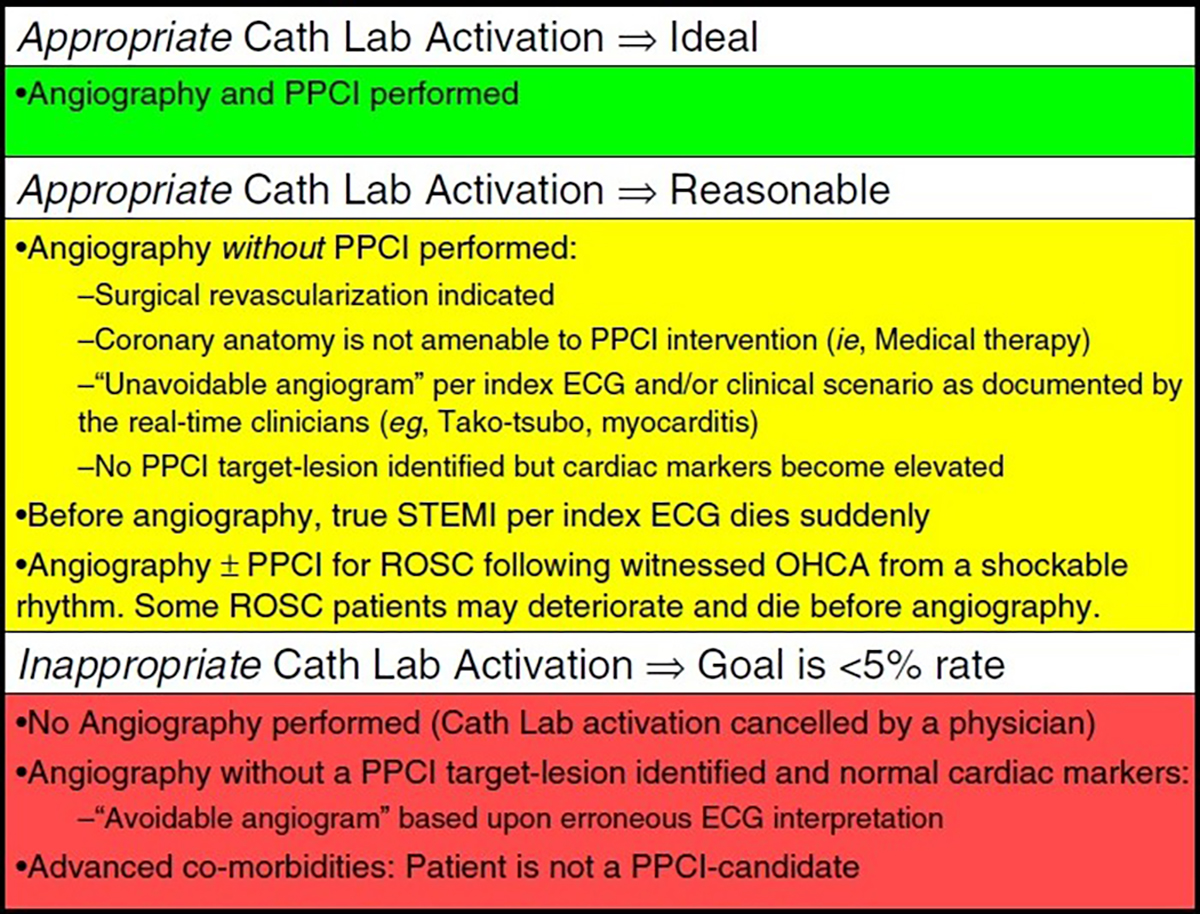
TCM is essentially indistinguishable from LAD occlusion and no criteria can be safely used to differentiate between the two conditions. An article in the American Heart Journal by Rokos et al. considers TCM an appropriate cardiac cath lab activation and “unavoidable angiogram” based on the 12-lead ECG findings.
References and further reading
British Heart Foundation (No Date) Takotsubo cardiomyopathy Online at: https://www.bhf.org.uk/heart-health/conditions/cardiomyopathy/takotsubo-cardiomyopathy [Accessed on 30/01/2016]
Buckley RG, Aks SE, Eshom JL, Rydman R, Schaider J and Shayne P (1994) ‘The pulse oximetry gap in carbon monoxide intoxication’ Ann Emerg Med 24 (2): 252-5 Online at: http://www.ncbi.nlm.nih.gov/pubmed/8037391
Harvard Health Publications (2001) Takotsubo cardiomyopathy (broken-heart syndrome) Online at: http://www.health.harvard.edu/heart-health/takotsubo-cardiomyopathy-broken-heart-syndrome [Accessed on 30/01/2016]
Edward Burns (No Date) Tako-tsubo cardiomyopathy Online at: http://lifeinthefastlane.com/ecg-library/tako-tsubo/ [Accessed 30/01/2016]
Sharkey SW, Lesser JR and Maron BJ (2011) ‘Takotsubo (Stress) Cardiomyopathy’ Circulation 124: e460-e462 Online at: http://circ.ahajournals.org/content/124/18/e460.full [Accessed 30/01/2016]
Tomich EB, Schraga E (2015) Takotsubo cardiomyopathy Online at: http://emedicine.medscape.com/article/1513631-overview#showall [Accessed on 30/01/2016]
Virani SS, Khan, AN, Mendoza CE, AC Ferreira and Marchena ED (2007) ‘Takotsubo Cardiomyopathy, or Broken-Heart Syndrome’ Tex Heart Inst Journal 34(1): 76-79 Online at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1847940/ [Accessed on 30/01/2016]
Rokos I, French W, Mattu A et al. Appropriate Cardiac Cath Lab activation: Optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. American Heart Journal. 2010;160(6):995-1003.e8. doi:10.1016/j.ahj.2010.08.011.