Guide to Understanding ECG Artifact
Mixed drug overdoses can cause dangerous cardiac complications, including sodium channel blockade, a condition that disrupts the heart’s electrical conduction and can quickly lead to wide-complex arrhythmias, seizures, severe acidosis, and shock. Recognizing these ECG changes early and initiating treatments such as sodium bicarbonate are critical skills for EMS providers and emergency clinicians managing overdose patients in the field. Developing the ability to identify and treat life-threatening cardiac rhythms is a core part of emergency care training, which is why many providers strengthen these skills through programs like BLS and ACLS certification courses that emphasize rapid assessment and intervention.
In this article, we’ll walk through a real-world EMS case involving a mixed drug overdose that led to severe sodium channel blockade. By examining the patient presentation, ECG findings, treatment decisions, and hospital course, you’ll see how early recognition and appropriate management can help prevent catastrophic outcomes.
Table of Contents
- Initial EMS Presentation of a Critically Ill Overdose Patient
- Suspected Substances and Risk of Mixed Drug Toxicity
- Primary Assessment and Initial Vital Signs
- ECG Findings Suggestive of Sodium Channel Blockade
- Seizures and Severe Acidosis in Overdose Patients
- Prehospital Management and Initial Interventions
- Why Sodium Bicarbonate is Used in Sodium Channel Blockade
- ECG Changes After Sodium Bicarbonate Administration
- Pathophysiology of Cocaine, Alcohol, and Dextromethorphan Co-Ingestion
- Respiratory Failure, Hypercapnia, and Shock Progression
- ICU Management and Hospital Course
- Challenges of Airway Management in Severe Acidosis
- Key Clinical Takeaways for Emergency and Prehospital Providers
Initial EMS Presentation of a Critically Ill Overdose Patient
30 minutes after going on-shift, an EMS unit is called to an apartment for an 18-year-old male experiencing seizures without any other details given. Upon arrival, EMS finds three high school-to-college aged individuals at varying levels of mental clarity, with a hefty supply of medications and alcohol on the kitchen counter.
A combination of mental fog and apprehension causes bystanders to offer little in the way of a history for the patient. Nevertheless, it is clear that the patient in question is not responding to verbal or physical stimulation and is exhibiting a slow respiratory pattern.
It’s important to note that this is a common occurrence in drug overdose scenarios: bystanders are often participants in polysubstance use and thus are afraid to offer any details for fear of incriminating themselves. It’s best to reassure bystanders that it’s essential for the patient’s safety and survival that they share what the patient ingested.
Suspected Substances and Risk of Mixed Drug Toxicity
At last, the friends of the patient offer the following: they and the patient were up all night drinking, partying, and ingesting multiple illicit substances. The patient was witnessed to have ingested large amounts of cocaine, “DXM” (dextromethorphan or ‘cough syrup’), alcohol, marijuana and nicotine. They all went to sleep at an unknown time, and no one stirred until a friend awoke to the patient seizing on the floor at 06:30 this morning, but no one knows how long the patient was down prior to being discovered seizing.
As an aside, polysubstance abuse is particularly dangerous because of the potentiating and prolonging effects of drug combinations. The combination of ingested substances makes the diagnosis complex given multiple drug interactions and the possibility of additional unknown substances ingested by the patient, leading to a wide spectrum of signs and symptoms without a clear or single origin.
Primary Assessment and Initial Vital Signs
You begin your assessment with ABC’s. The patient is nonresponsive to stimuli, has a weak and agonal respiratory effort, large sluggish pupils, and a faint and slow carotid pulse. A brief survey also reveals significant pallor and central cyanosis, but the patient is paradoxically hot to the touch.
The patient’s initial vital signs and exam are as follows:
- HR: 60/min
- RR: 6/min
- SpO2: <50%
- NIBP: 66/34 [44]
- Pupils: 6mm bilaterally, extremely sluggish
- BGL: 90mg/dl
- Temp: 38.5 C (101.3F)
The patient is clearly experiencing hypoxia, hypotension, hyperthermia and bradypnea. While hyperthermia is expected in cocaine overdose, the hypotension and bradypnea are particularly ominous since cocaine is a stimulant - in contrast, this patient’s blood pressure has bottomed out, representing a spiral toward cardiovascular and respiratory collapse due to the potentiated sodium-channel-blocking properties of cocaine and DXM.
Crews begin administering high-quality 2-person BVM ventilation, utilizing a jaw thrust while inserting an OPA, and positioning the patient with padding behind the head to support a proper ear-to-sternal-notch alignment . Intravenous access, fluid resuscitation, reoxygenation, and basic cardiac monitoring is being maintained while extrication from the apartment is coordinated.
ECG Findings Suggestive of Sodium Channel Blockade
The following rhythm is observed on the monitor. Shortly after, the patient has a generalized seizure which lasts approximately 5 minutes.
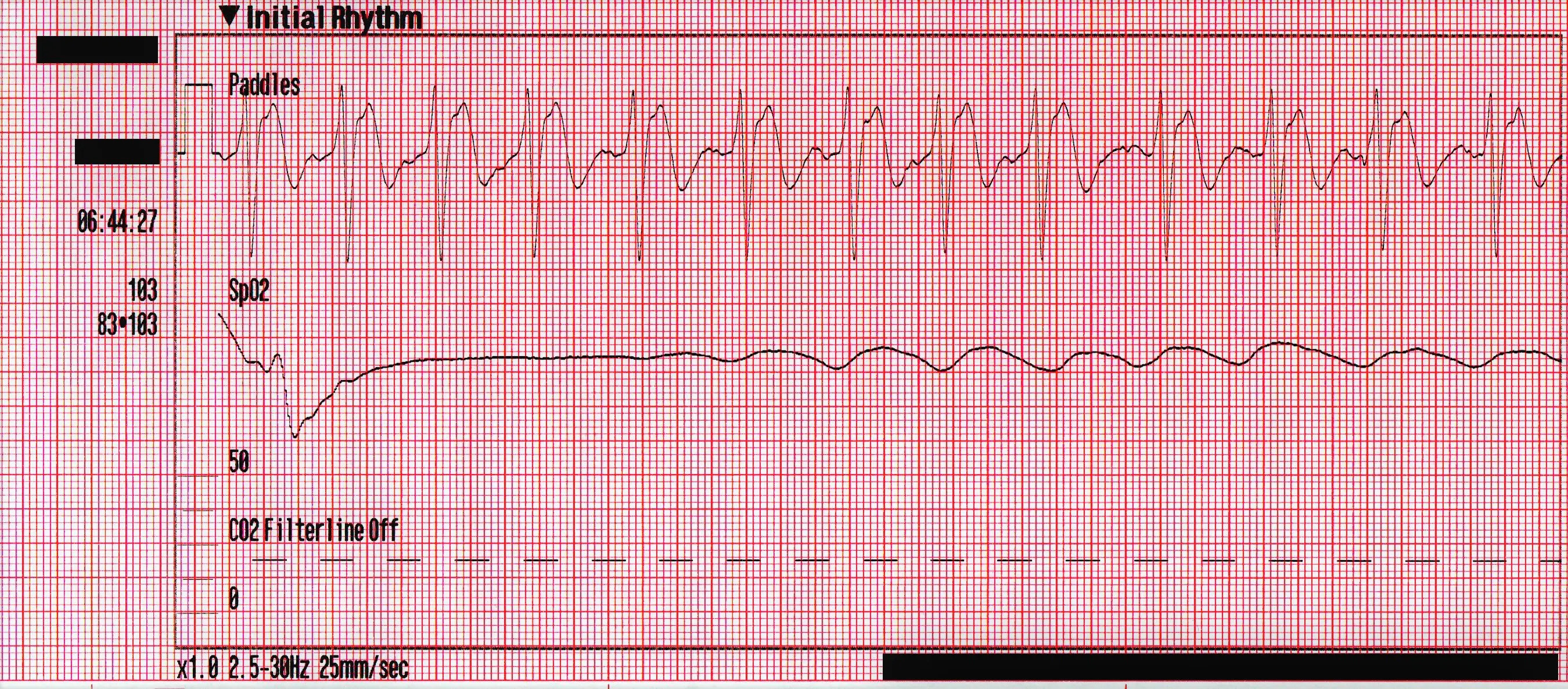
Once in the ambulance, passive cooling is initiated, and a supraglottic airway is placed. His blood pressure has improved to 87/44 [59], his SpO2 remains in the mid-80’s, and his initial ETCO2 is 86mmHg. The following 12-lead is then acquired:
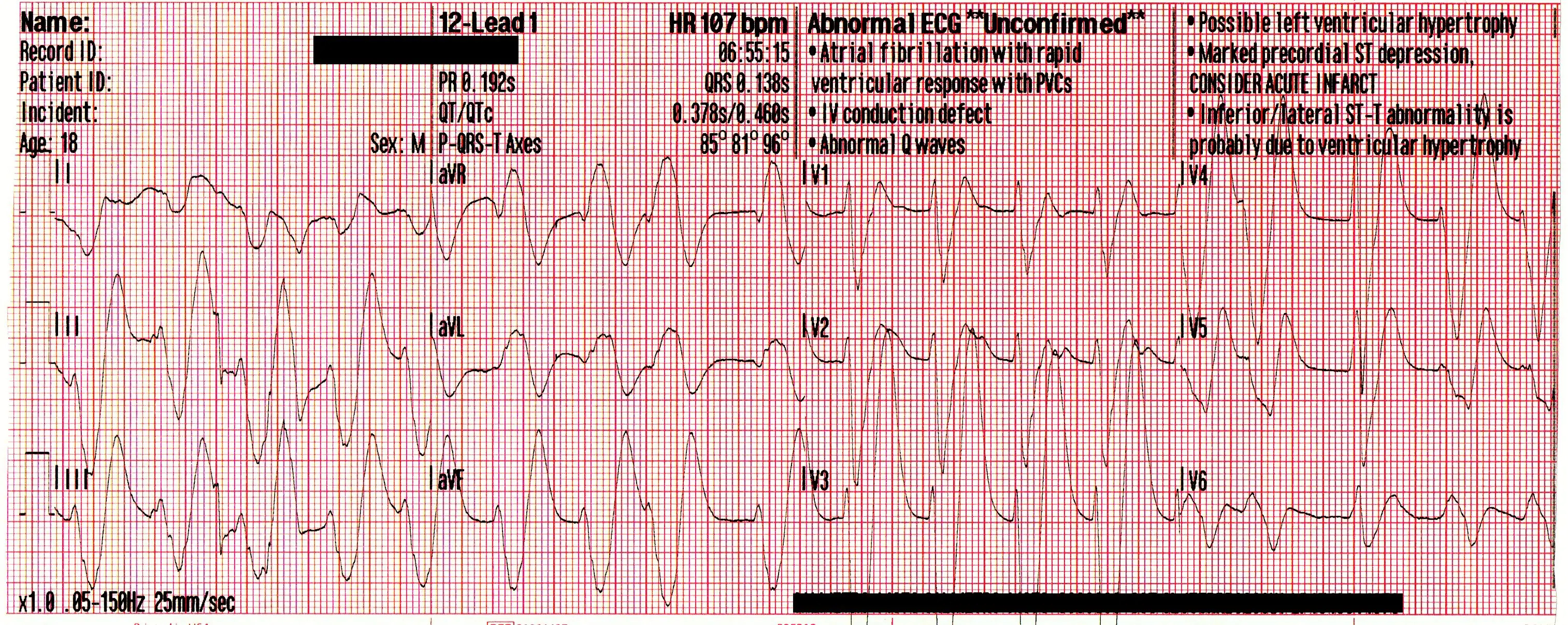
A significant wide-complex tachycardia that is irregularly irregular, with an extreme right axis deviation and a massive terminal R-wave in aVR measuring 10mm. Given the patient’s suspected ingestions and current clinical condition, this ECG should be considered pathognomonic for severe sodium-channel blockade being complicated by extreme acidosis.
Because of the cocaine sodium channel blockade, ECG findings will show wide complex tachycardia due to ventricular sodium channel blockage which prevents faster conduction through the His-Purkinje system. The danger here is the increased risk of ventricular tachycardia or “R-on-T” phenomenon (leading to ventricular fibrillation). Additionally, extreme axis deviation and a prominent R wave in aVR are also caused by sodium channel blockage which affects the right bundle branch, redirecting the direction of depolarization across the cardiac muscle myocytes which causes the ECG tracing to deviate. These findings together indicate cocaine toxicity complicated by polysubstance use.
Seizures and Severe Acidosis in Overdose Patients
So why is our patient seizing? Not only has the patient ingested pro-convulsant drugs (cocaine/dextromethorphan/alcohol), but they have also developed multiple conditions that lower their seizure threshold including hypoxia, hypercapnia and acidosis. These conditions adjust the excitability of nerve cells, making them increasingly prone to aberrant discharges leading to seizure activity.
This becomes a dangerous “positive-feedback loop” as prolonged seizures with sustained muscle contractions increase lactic acidosis and deplete glucose stores, both of which lower the seizure threshold. Additionally, a lower blood pH is associated with increased cocaine binding to sodium channels which further slows electrical conduction across cardiac myocytes, placing the patient at greater risk for conduction abnormalities.
Prehospital Management and Initial Interventions
Initial management of the patient is aimed at supporting ABC’s. Supplemental oxygen with ventilation should be given to the hypoxic patient, with intubation performed if necessary in the setting of airway compromise.
Regarding circulatory support, hypotension should first be addressed with normal saline or an isotonic solution, typically 2-3 liters, followed by vasopressors if unresolved.
Early ventilation and oxygen supplementation are necessary, not simply as a supportive measure, but to reverse acidosis via CO2 removal (with mechanical ventilation) which reverses the sodium-channel blockade and decreases the excitability of neuronal clusters for maintaining a proper seizure threshold. Additionally, supplemental oxygen increases oxygen saturation, combating cardiac hyperexcitability and the risks of dangerous arrhythmias while promoting aerobic metabolism which slows the production of lactic acid.
Why Sodium Bicarbonate is Used in Sodium Channel Blockade
Intravenous sodium bicarbonate acts as a treatment for overdose in a patient like ours via a multi-pronged attack. Following administration, there’s a rapid dissociation of NaHCO3 into Na + HCO3. The extra sodium acts to “overload” the blocked sodium-channels, while the bicarbonate acts as a buffer and binds with free hydrogen (H+) ions to form Carbonic Acid (H2CO3) which then dissociates into water and carbon dioxide, expressed as HCO3 + H → H2CO3 → H2O + CO2. This allows for respiratory correction of the acidosis, and the subsequent alkalinization of the blood helps to reduce the channel-toxic effects of the cocaine. It should be noted, however, that this requires an increased rate of ventilation to ensure adequate elimination of the rising CO2 levels that will follow.
In the setting of wide complex tachycardia with overdose, ECG tracings require differentiation via sodium bicarbonate, which plays an essential role in treating cocaine-related cardiotoxicity since it provides both therapeutic and diagnostic effects for the patient: if the patient is experiencing a true ventricular tachycardia, then the QRS width will not shorten with the administration of sodium bicarbonate. However, if the patient’s widened QRS is due to cardiotoxic effects of cocaine and other sodium-channel blocking drugs, then the QRS will begin to shorten, reducing the patient’s threshold for dangerous arrhythmias.
ECG Changes After Sodium Bicarbonate Administration
Returning to our scenario, paramedics identified the patient’s above arrhythmia to most-likely be a complication of the cocaine toxicity, and treatment was aimed at hyperventilation and administration of intravenous sodium bicarbonate (NaHCO3) to correct the acidosis.
The following 12-lead was recorded following the administration of one amp of 50mEq of NaHCO3 with ongoing attempts at hyperventilation.
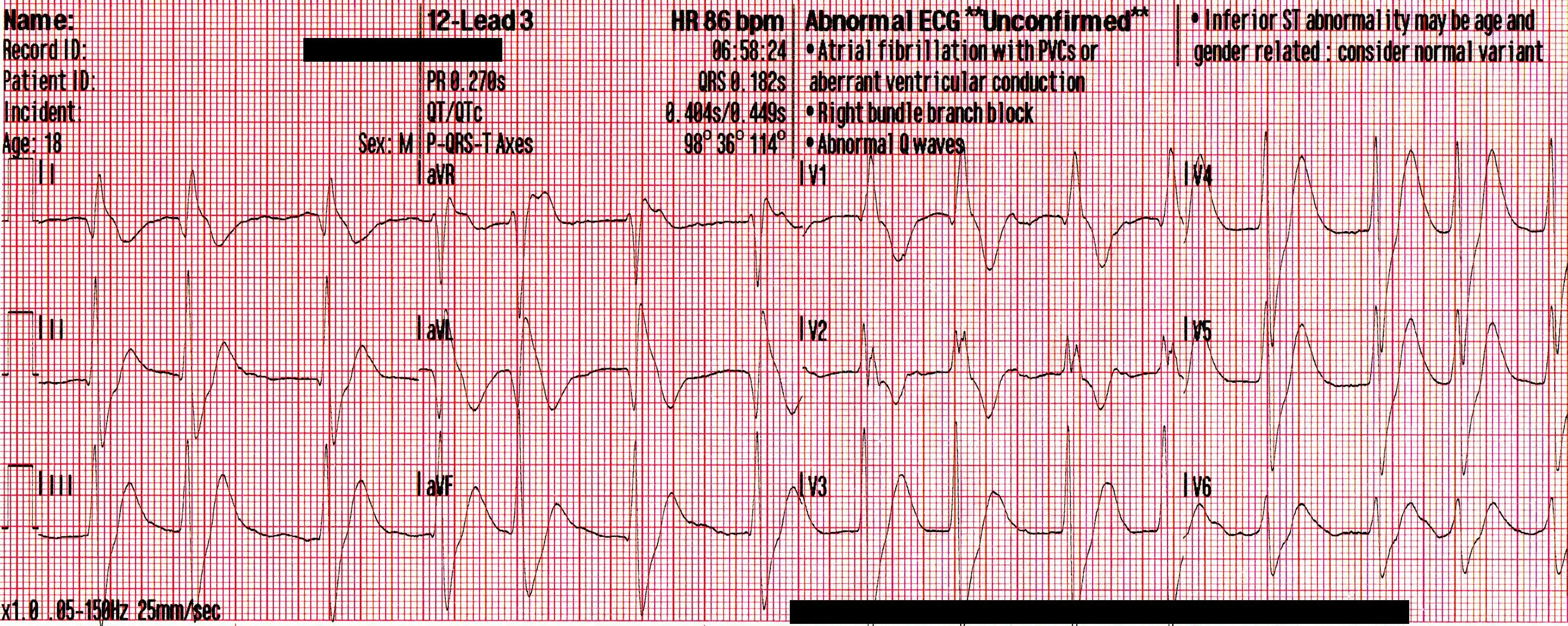
An irregularly-irregular wide-complex rhythm, with an apparent RBBB pattern and peaked T-waves reminiscent of hyperkalemia. This is an improvement, but there are still signs of significant sodium channel blockade.
With supplemental oxygenation and mechanical ventilation, the patient’s SpO2 improved to 100%, his blood pressure remained 85/35 [55], and despite being ventilated at a rate of 30/minute, his ETCO2 remained 86mmHg. Another 50mEq of NaHCO3 is administered, and the following 12-lead is acquired:
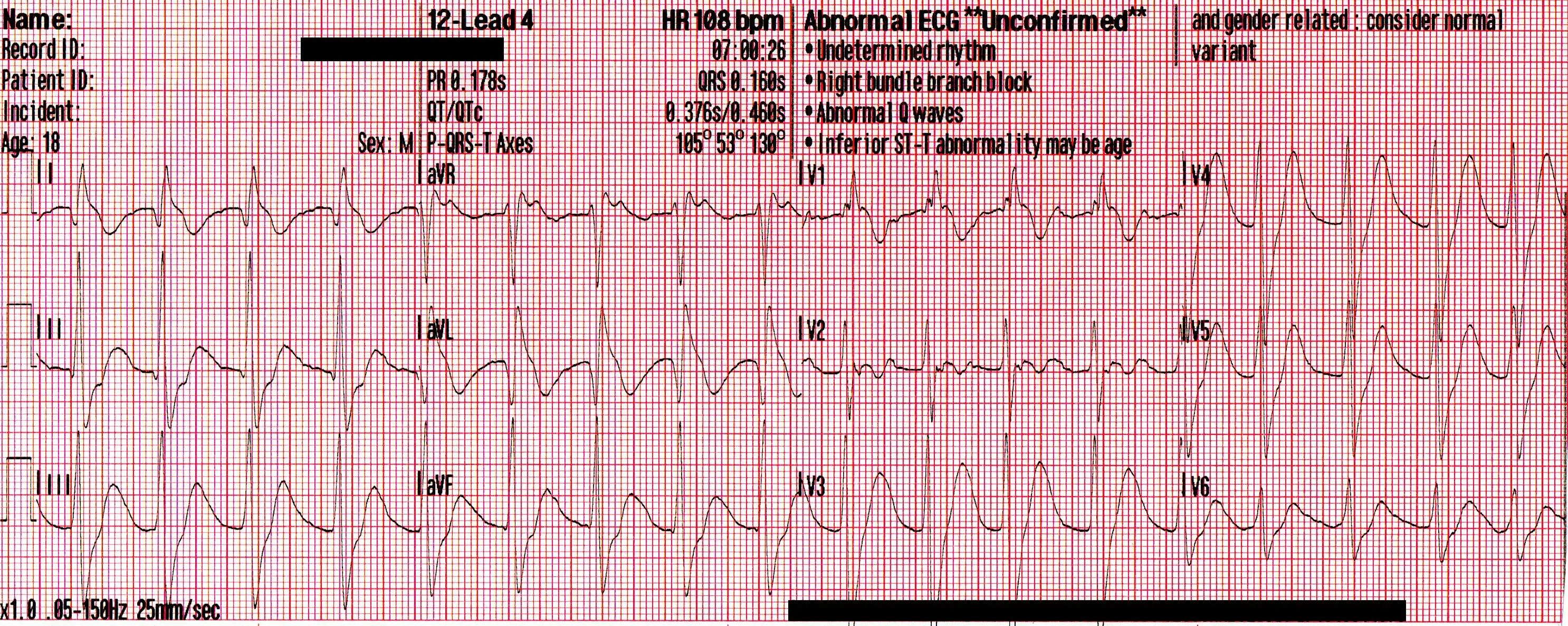
A regular, wide-complex rhythm, with a similar QRS morphology to the previous 12-lead. The QRS is gradually narrowing but remains pathological.
As discussed in the prior section, narrowing QRS complexes confirm the diagnosis of a cocaine-induced sodium channel blockade that is manageable with administration of sodium bicarbonate and oxygen supplementation with CO2 removal (via increased ventilation). When following this treatment protocol, serial ECG monitoring is essential to confirm both diagnosis and treatment of this condition.
Pathophysiology of Cocaine, Alcohol, and Dextromethorphan Co-Ingestion
This patient’s presentation can likely be explained by the complex interaction between each of the substances that were ingested. Cocaine mixed with alcohol forms cocaethylene when metabolized by the liver, a substance that’s significantly more cardiotoxic and possesses a half-life 3-5 times that of cocaine alone. Amongst its multiple mechanisms, it acts as a Class Ic sodium-channel blocker which is represented on the ECG as a progressive widening of the QRS complexes and the development of an extreme rightward axis in the frontal plane. These channel-toxic effects are amplified by increases in heart rate and decreases in pH.
The deleterious effects of the cocaethylene, combined with the ingestion of significant amounts of dextromethorphan, an antitussive and a NMDA-receptor antagonist, would likely result in euphoria, tachycardia, hypertension, dissociation, a decreasing level of consciousness, and potentially severe serotonin syndrome. Additionally, their synergistic effect in a setting of acidosis would lead to increased sodium-channel binding, inhibition of sodium currents, decreased cardiac conduction, widened QRS and decreased myocardial contractility, placing the patient at high risk for arrhythmias and cardiogenic shock.
Respiratory Failure, Hypercapnia, and Shock Progression
Respiratory depression in any setting is deadly, not simply because oxygen saturation levels decrease, but also because CO2 is retained. CO2 is a major driver of acidosis in pH balance and, as the body retains more CO2, pH will slide down into acidotic territory.
A disrupted respiratory drive leads to hypercapnia and worsening acidosis which, combined with hyperthermia and polysubstance abuse, places the patient at a decreased seizure threshold and at risk for arrhythmias. Left unchecked, hypoxia with hypercapnia and acidosis would predictably spiral into a self-perpetuating loop, inevitably resulting in profound shock and hemodynamic collapse.
ICU Management and Hospital Course
Returning to our patient, the crew arrived at the hospital shortly after a second amp of NaHCO3 was given. The ED staff continued administering subsequent doses of NaHCO3 while initiating a peripheral vasopressor (norepinephrine). The patient was then intubated and placed on a ventilator, after which initial arterial blood gases revealed a pH of <6.8, pCO2 of >100mmHg, and a lactate of >20mmol/L. He was sent for a CT-head, which revealed no obvious findings of hemorrhage or anoxic brain injury.
He was admitted to ICU and his repeat ABG thirty minutes later revealed an improved pH of 7.28 and pCO2 of 48mmHg.
Even after a patient is initially stabilized, aggressive supportive care is necessary to reverse the spiral of hypoxia, hypercapnia and acidosis. This is because the ingested polysubstance cocktail has a prolonged half-life which must be counteracted until the sodium-channel blocking substances are metabolized. Additionally, sodium-channel blockade can be counteracted with target alkalinization using techniques such as hyperventilation and NaCO3 administration which maintains the pH in an elevated range of 7.45-7.55 to maximize sodium channel availability.
Challenges of Airway Management in Severe Acidosis
Intubation of this patient would also prove delicate, since critical hypotension and acidosis would likely be worsened by the use of most induction agents or paralytics, forcing providers to classify this as a physiologically difficult airway. A physiologically difficult airway refers to a patient with severe conditions such as profound hypoxemia, hypotension and acidosis that places them at a high risk of cardiovascular collapse during induction and intubation.
For this reason, airway management should likely be accomplished using a resuscitate-before-you-intubate approach. Fluid resuscitation should be well underway, push-dose pressors should be at the ready and providers should be aware that there’s a high-likelihood of this patient requiring vasopressor support despite receiving a 20ml/kg crystalloid bolus.
Additionally, regarding induction agents for intubating patients with cocaine toxicity, succinylcholine should absolutely be avoided since, in combination, the cardiotoxic effects of the cocaine and the paralytic effects of succinylcholine will both be prolonged. On top of that, the drug may also worsen hyperkalemia in the setting of hyperthermia and rhabdomyolysis. Alternative paralytics such as rocuronium may be used instead.
Key Clinical Takeaways for Emergency and Prehospital Providers
In summation, in a mixed overdose setting, early recognition of sodium channel blockade is paramount to prevent cardiovascular and seizure complications. ECG interpretation with rapid diagnostic administration of bicarbonate therapy is crucial for differentiating between prolonged QRS from sodium channel blockade and ventricular tachycardia, with subsequent dosing of bicarbonate to maximize sodium channel availability.
In conclusion, the critically ill mixed-overdose patient requires aggressive yet calculated emergency management from first responders and physicians alike. A clinical understanding of the pathophysiology, as well as the implications of each aspect of treatment, is vitally important in caring for each of these patients.
Familiarity and confidence in treating conditions like this are achieved only by training with simulated exposure. BLS Certification training and ACLS Certification training assist providers to recognize deterioration and provide immediate and effective treatment. Consider bolstering your expertise by signing up for a certification or recertification course today!
References
Hoffman RS. Cocaine: Acute intoxication. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate; 2024. Accessed February 26, 2024. https://www.uptodate.com/contents/cocaine-acute-intoxication
Hoffman RS. Treatment of patients with cocaine-induced arrhythmias: bringing the bench to the bedside. Br J Clin Pharmacol. 2010;69(5):448-457. doi:10.1111/j.1365-2125.2010.03632.x
McCord J, Jneid H. Clinical manifestations, diagnosis, and management of the cardiovascular complications of cocaine use. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate; 2024. Accessed February 26, 2024. https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-management-of-the-cardiovascular-complications-of-cocaine-use
O’Leary ME, Hancox JC. Role of voltage-gated sodium, potassium and calcium channels in the development of cocaine-associated cardiac arrhythmias. Br J Clin Pharmacol. 2010;69(5):427-442. doi:10.1111/j.1365-2125.2010.03629.x
Traub SJ. Initial management of the critically ill adult with an unknown overdose. In: Post TW, ed. UpToDate. Waltham, MA: UpToDate; 2024. Accessed February 26, 2024. https://www.uptodate.com/contents/initial-management-of-the-critically-ill-adult-with-an-unknown-overdose

{kind=link}