
Cocaine Overdose Presents with Wide Complex Tachycardia
A 45 year old male with unknown medical history was taken into police custody under concern for trafficking illegal drugs.
While he was in the back of the squad car he told the police he had swallowed a large amount of cocaine and may need to go to the hospital. Not long afterwards he became unresponsive and paramedics were called to the scene.
Paramedics found the patient minimally arousable.
Vital signs were assessed.
- RR: 12
- HR: 130
- NIBP: 140/69
- SpO2: 95% on room air
- Temp: 36.8 C / 98.2 F
- BGL: 137
The cardiac monitor shows “sinus tachycardia” (the prehospital ECG is unavailable).
During transport paramedics witness tonic-clonic seizure activity and 2 mg of IV lorazepam is given.
On arrival in the Emergency Department the airway is intact, respirations are shallow, and there is no response to painful stimuli. A nasopharyngeal airway is placed, the patient is ventilated with a bag valve mask, and then intubated via rapid sequence induction.
A 12-lead ECG is acquired.
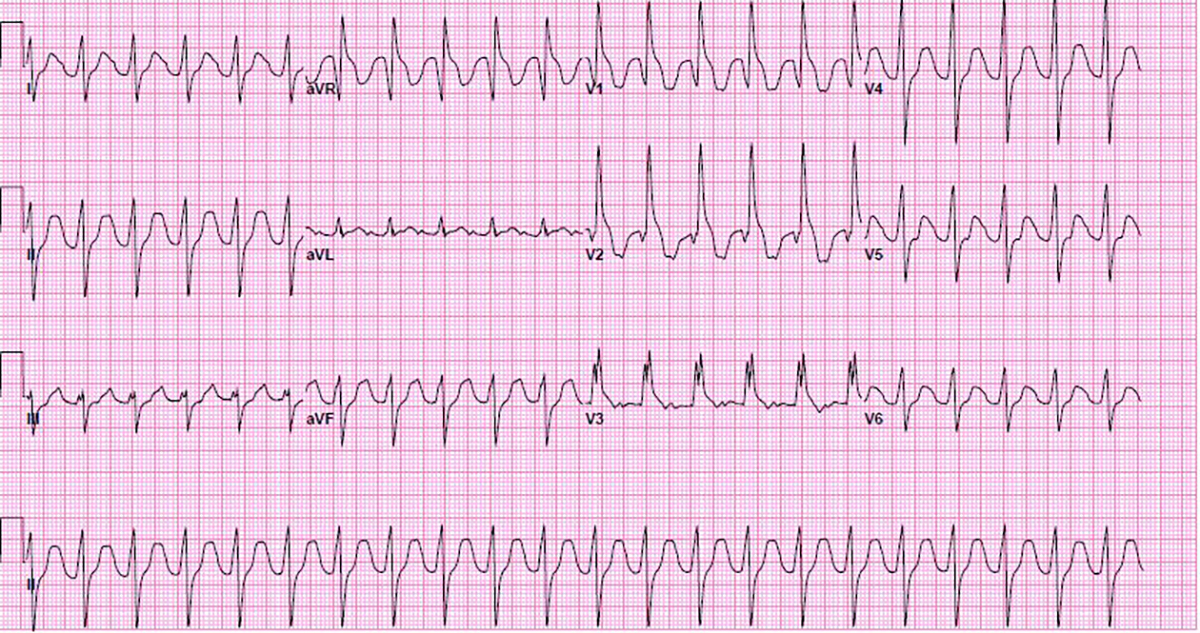
The QRS is wide at 138 ms. The QTc is prolonged at 596 ms. P waves can be seen in leads aVL and V3. This is most likely sinus tachycardia with toxicologic widening of the QRS.
200 mEq sodium bicarb is given and another 12-lead ECG is obtained.
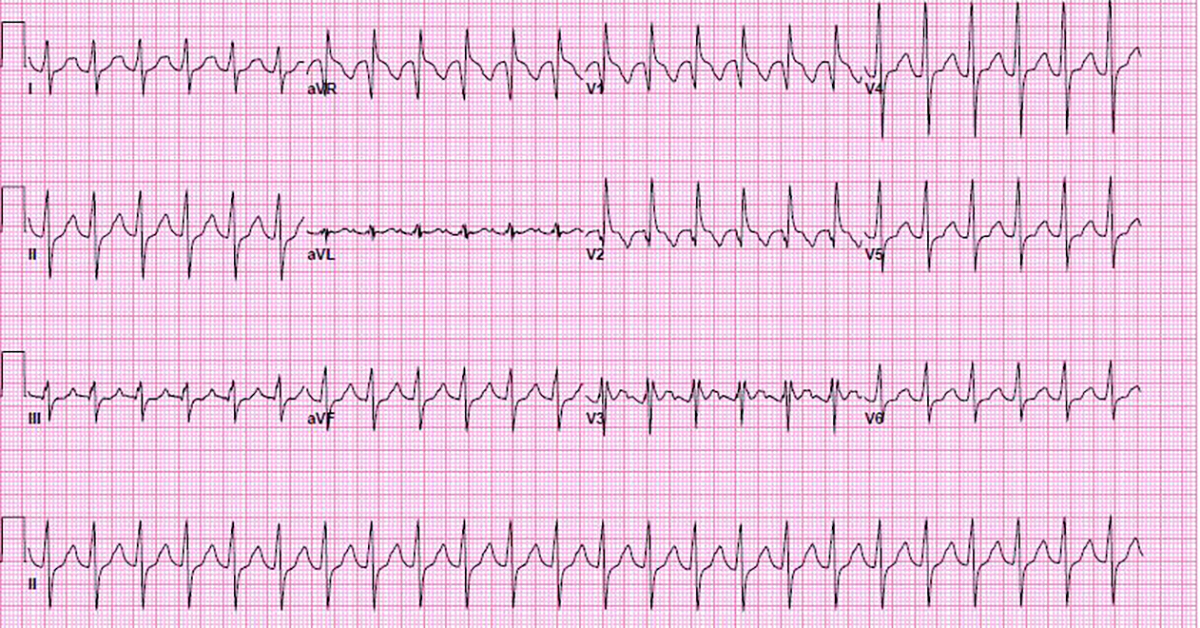
The QRS is now 130 ms and the QTc is 587ms.
An additional 200 mEq of sodium bicarb is given and the patient is started on a sodium bicarb drip, 150 mEq in 1,000 mL at 150 mL/hr.
30 minutes later the 12-lead ECG is repeated.
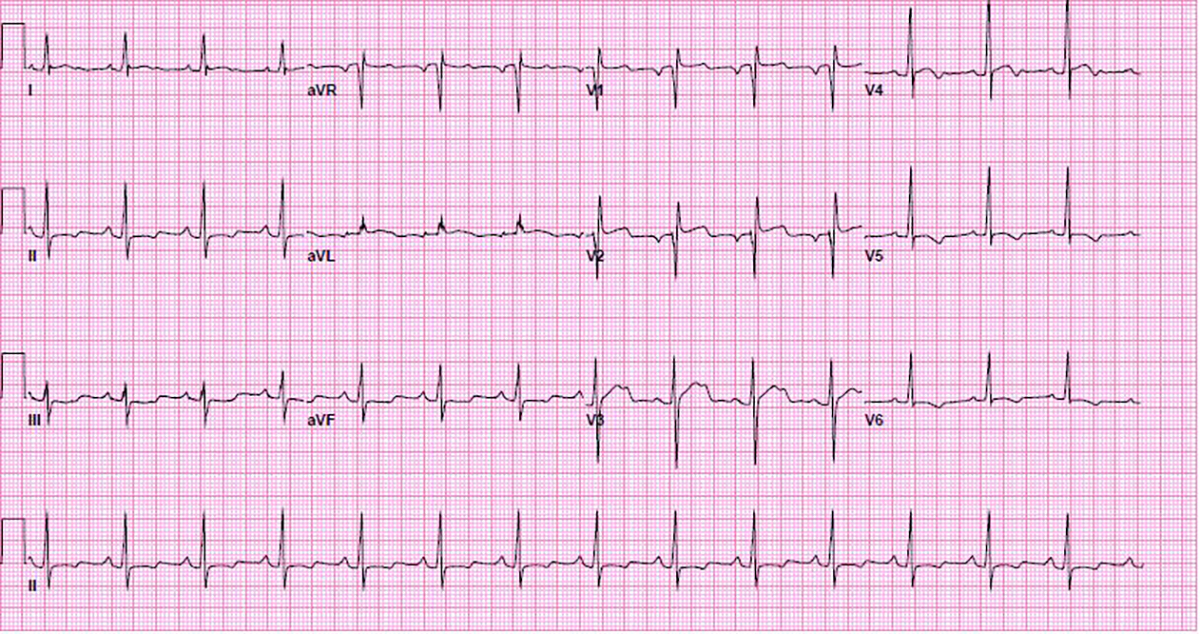
The QRS is now 90 msec with QTc 464 msec.
Now the QRS shows a normal duration but there are some troubling ECG findings.
ST-segment elevation is noted in the right precordial leads (V1-V3) and the high lateral leads (I and aVL), with ST-segment depression in the inferior leads (II, III, and aVF). There are Q-waves in leads V1 and V2 with a QR pattern.
This was thought to be secondary to patient’s cocaine use and not from thrombotic disease so the cardiac cath lab was not immediately activated. Cardiac biomarkers remained negative, and the ST-segments normalized during hospitalization.
Discussion
- Cocaine acts like a Class I antiarrhythmic which causes sodium channel blockade and widening of the QRS complex.
- Treatment of toxicologic widening of the QRS consists of sodium bicarbonate (the sodium helps to overcome the blockade caused by the cocaine).
- If QRS does not improve with sodium bicarbonate an alternative diagnosis other than toxicologic widening of the QRS should be considered.
- Cocaine can also cause QT prolongation via blockade of the K+ rectifier channels.
- Other cardiovascular events such as coronary artery spasm, myocardial infarction, hemorrhagic stroke, and aortic dissection related to sympathomimetic properties of cocaine should be considered in the differential diagnosis.


Comments