CPR First? Or Defibrillation First?
Ventricular Fibrillation is considered the most favorable cardiac arrest rhythm, and if treated promptly can result in ROSC with a favorable neurological outcome. Most survival rates are reported using witnessed arrest with a shockable rhythm as opposed to asystole or PEA, as the outcomes of these rhythms are comparatively very poor.
The Resuscitation Academy mantra “everyone in VF survives” has been adopted by many EMS systems around the world to emphasize that these patients can and do survive, and it’s up to us to save them.
Major advances have been made over the past 10 years but CPR and defibrillation are still the bedrock of resuscitation science. The attributes of high-quality CPR were re-affirmed in the 2015 AHA ECC Guidelines.
- Ensuring adequate rate (100-120)
- Ensuring adequate depth (2 to 2.4” or 5 to 6 cm)
- Allowing full chest recoil (avoid leaning)
- Minimizing interruptions to chest compressions
- Avoiding excessive ventilations
Is CPR Before Defibrillation Dogmatic?
In the context of a witnessed arrest by a trained first responder or bystander who has an AED or manual defibrillator, the importance of early defibrillation is irrefutable. We have been told repeatedly that early defibrillation saves lives.
I initially began my research under the assumption that providing 1.5 to 3 minutes of CPR before defibrillation provides oxygen and nutrients to the heart therefore making defibrillation more likely to be successful. However, recent evidence suggests that performing chest compressions while setting up the defibrillator and charging the capacitor may be adequate.
A “CPR first” approach is rooted in evidence suggesting the existence of 3 time-sensitive phases of VF arrest.
- Electrical phase (0-4 minutes)
- Circulatory phase (5-10 minutes)
- Metabolic Phase (> 10 minutes)
Researchers suggested that a period of CPR prior to defibrillation might confer a benefit during the so-called “circulatory phase” of the cardiac arrest.
Evolution of American Heart Association Recommendations
Because it is rare for EMS to arrive on scene during the electrical phase, the 2005 AHA ECC Guidelines made this recommendation:
- When an out-of-hospital cardiac arrest is not witnessed by EMS personnel, they may give about 5 cycles of CPR before checking the ECG rhythm and attempting defibrillation (Class IIb). One cycle of CPR consists of 30 compressions and 2 breaths. When compressions are delivered at a rate of about 100 per minute, 5 cycles of CPR should take roughly 2 minutes (range: about 1½ to 3 minutes). This recommendation regarding CPR prior to attempted defibrillation is supported by 2 clinical studies (LOE 2, LOE 3) of adult out-of-hospital VF SCA. In those studies when EMS call-to-arrival intervals were 4 to 5 minutes or longer, victims who received 1½ to 3 minutes of CPR before defibrillation showed an increased rate of initial resuscitation, survival to hospital discharge, and 1-year survival when compared with those who received immediate defibrillation for VF SCA. One randomized study, however, found no benefit to CPR before defibrillation for non-paramedic-witnessed SCA.
Fast forward 10 years to the 2015 Guidelines.
- Observational clinical studies and mechanistic studies in animal models suggest that CPR under conditions of prolonged untreated VF might help restore metabolic conditions of the heart favorable to defibrillation…others have suggested that prolonged VF is energetically detrimental to the ischemic heart, justifying rapid defibrillation attempts regardless of the duration of arrest.
Evidence summary
- Five RCTs, 4 observational cohort studies, 3 meta-analyses, and 1 subgroup analysis of an RCT addressed the question of CPR before defibrillation. The duration of CPR before defibrillation ranged from 90 to 180 seconds, with the control group having a shorter CPR interval lasting only as long as the time required for defibrillator deployment, pad placement, initial rhythm analysis, and AED charging. These studies showed that outcomes were not different when CPR was provided for a period of up to 180 seconds before attempted defibrillation compared with rhythm analysis and attempted defibrillation first for the various outcomes examined, ranging from 1-year survival with favorable neurologic outcome to ROSC. Subgroup analysis suggested potential benefit from CPR before defibrillation in patients with prolonged EMS response intervals (4 to 5 minutes or longer) and in EMS agencies with high baseline survival to hospital discharge, but these findings conflict with other subset analyses. Accordingly, the current evidence suggests that for unmonitored patients with cardiac arrest outside of the hospital and an initial rhythm of VF or pVT, there is no benefit from a period of CPR of 90 to 180 seconds before attempted defibrillation.
Specifically, the ROC PRIMED trial concluded that:
- Among patients who had an out-of-hospital cardiac arrest, we found no difference in the outcomes with a brief period, as compared with a longer period, of EMS-administered CPR before the first analysis of cardiac rhythm.
The ROC Investigators subsequently found that EMS systems with a VF survival rate < 20% appeared to do better with an “analyze first” strategy. Conversely, EMS systems with a VF survival rate > 20% appeared to do better with a “analyze late” strategy.
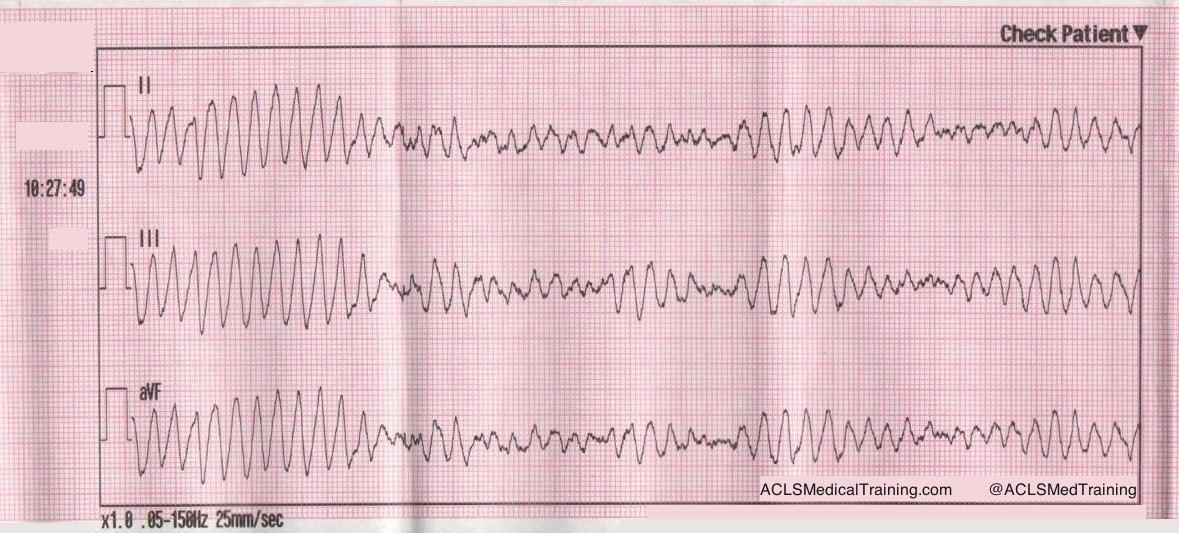
Can the VF Waveform Determine the Likelihood of Successful Defibrillation?
Ventricular fibrillation sometimes begins as ventricular tachycardia, and if left untreated deteriorates into fine VF. Fine VF predictably results in conversion to asystole or continued VF, but rarely to a perfusing rhythm.
Berg et al. performed a randomized, controlled trial using animals. After inducing VF in swine for 8 minutes, they were randomly assigned to either immediate defibrillation, or defibrillation provided after 90 seconds of CPR. Nine out of 15 attained ROSC in the CPR first group, and zero out of 15 who were defibrillated first resulted in ROSC. Their conclusion?
- Pre-countershock CPR can result in substantial physiologic benefits and superior response to initial defibrillation attempts compared with immediate defibrillation in the setting of prolonged ventricular fibrillation.
Additionally, they determined there was a mathematical relationship between the VF waveform and chances of successful defibrillation. The animals who received CPR first had a much higher median frequency, and a much higher rate of ROSC than those that did not.
In the field, whether or not VF is “fine” or “coarse” is typically based on visual inspection of the waveform. What if there was a way to accurately determine which patients would benefit from defibrillation and those that would not, thus eliminating unnecessary pauses and ineffective shocks?
Callaway et al. and Eftestol et al. supported the theory that VF frequency and amplitude could be used to determine which patients will respond to countershock.
Eftestol et al. concluded:
- CPR done by professionals can improve the chance for ROSC and ultimate survival of patients with prolonged cardiac arrest and significantly deteriorated myocardium. This study also indicates that CPR periods of 3 minutes might be better for the myocardium than shorter periods. Finally, together with the studies showing rapid deterioration of the myocardium in even a few seconds without CPR after a cardiac arrest, it gives the important message that periods without CPR (for ECG analysis, defibrillation charging, pulse checks, intubation attempts, etc) should be kept to a minimum. This is frequently not the case clinically.
As promising as this may have seemed, an article in Circulation by Freese et al. evaluated the theory of defibrillation based on waveform analysis, and the results were disappointing.
- Use of a waveform analysis algorithm to guide the initial treatment of out-of-hospital cardiac arrest patients presenting in VF did not improve overall survival compared with a standard shock-first protocol. Further study is recommended to examine the role of waveform analysis for the guided management of VF.
The Bottom Line
The totality of the evidence suggests that defibrillation as soon as practicable (with the caveat that high quality chest compressions are performed while setting up the defibrillator) is equivalent to a prescribed interval of CPR prior to the first shock in most instances.
EMS systems that measure the “patient’s side to first shock” interval know that it usually takes at least 1 minute to power on the defibrillator, extend the cables, attach the pads, charge the capacitor, and deliver the shock. During that interval, there’s no reason that the patient can’t receive continuous chest compressions.
One benefit to emphasizing a “shock as soon as possible” approach is that it’s the same for EMS-witnessed cardiac arrest.
Alternatively, defibrillation can be delivered after the first 2-minute cycle. It seems likely that CPR quality plays a more important role than the exact timing of the first shock.
References
Baker PW, Conway J, Cotton C, Ashby DT, Smyth J, Woodman RJ, Grantham H; Clinical Investigators. Defibrillation or cardiopulmonary resuscitation first for patients with out-of-hospital cardiac arrests found by paramedics to be in ventricular fibrillation? A randomised control trial. Resuscitation. 2008;79:424–431. doi: 10.1016/j.resuscitation.2008.07.017.
Bradley SM, Gabriel EE, Aufderheide TP, Barnes R, Christenson J, Davis DP, Stiell IG, Nichol G; Resuscitation Outcomes Consortium Investigators. Survival increases with CPR by Emergency Medical Services before defibrillation of out-of-hospital ventricular fibrillation or ventricular tachycardia: observations from the Resuscitation Outcomes Consortium. Resuscitation. 2010;81:155–162. doi: 10.1016/j. resuscitation.2009.10.026.
Cobb LA, Fahrenbruch CE, Walsh TR, Copass MK, Olsufka M, Breskin M, Hallstrom AP. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out-of-hospital ventricular fibrillation. JAMA. 1999;281:1182–1188.
Freese J, Jorgenson D, Liu P et al. Waveform Analysis-Guided Treatment Versus a Standard Shock-First Protocol for the Treatment of Out-of-Hospital Cardiac Arrest Presenting in Ventricular Fibrillation: Results of an International Randomized, Controlled Trial. Circulation. 2013;128(9):995-1002. doi:10.1161/circulationaha.113.003273.
Gilmore C, Rea T, Becker L, Eisenberg M. Three-Phase Model of Cardiac Arrest: Time-Dependent Benefit of Bystander Cardiopulmonary Resuscitation. The American Journal of Cardiology. 2006;98(4):497-499. doi:10.1016/j.amjcard.2006.02.055.
Hayakawa M, Gando S, Okamoto H, Asai Y, Uegaki S, Makise H. Shortening of cardiopulmonary resuscitation time before the defibrilla- tion worsens the outcome in out-of-hospital VF patients. Am J Emerg Med. 2009;27:470–474. doi: 10.1016/j.ajem.2008.
Huang Y, He Q, Yang LJ, Liu GJ, Jones A. Cardiopulmonary resuscitation (CPR) plus delayed defibrillation versus immediate defibrillation for out-of-hospital cardiac arrest. Cochrane Database Syst Rev. 2014;9:CD009803. doi: 10.1002/14651858.CD009803.pub2.
Jacobs IG, Finn JC, Oxer HF, Jelinek GA. CPR before defibrillation in out-of-hospital cardiac arrest: a randomized trial. Emerg Med Australas. 2005;17:39–45. doi: 10.1111/j.1742-6723.2005.00694.x.
Kleinman M, Brennan E, Goldberger Z et al. Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality. Circulation. 2015;132(18 suppl 2):S414-S435. doi:10.1161/cir.0000000000000259.
Koike S, Tanabe S, Ogawa T, Akahane M, Yasunaga H, Horiguchi H, Matsumoto S, Imamura T. Immediate defibrillation or defibrillation after cardiopulmonary resuscitation. Prehosp Emerg Care. 2011;15:393–400. doi: 10.3109/10903127.2011.569848.
Ma MH, Chiang WC, Ko PC, Yang CW, Wang HC, Chen SY, Chang WT, Huang CH, Chou HC, Lai MS, Chien KL, Lee BC, Hwang CH, Wang YC, Hsiung GH, Hsiao YW, Chang AM, Chen WJ, Chen SC. A randomized trial of compression first or analyze first strategies in patients with out-of-hospital cardiac arrest: results from an Asian community. Resuscitation. 2012;83:806–812. doi: 10.1016/j.resuscitation.2012.01.009.
Meier P, Baker P, Jost D, Jacobs I, Henzi B, Knapp G, Sasson C. Chest compressions before defibrillation for out-of-hospital cardiac arrest: a meta-analysis of randomized controlled clinical trials. BMC Med. 2010;8:52. doi: 10.1186/1741-7015-8-52.