A 45 year old male with unknown medical history was taken into police custody under concern for trafficking illegal drugs.
While he was in the back of the squad car he told the police he had swallowed a large amount of cocaine and may need to go to the hospital. Not long afterwards he became unresponsive and paramedics were called to the scene.
Paramedics found the patient minimally arousable.
Vital signs were assessed.
RR: 12
HR: 130
NIBP: 140/69
SpO2: 95% on room air
Temp: 36.8 C / 98.2 F
BGL: 137
The cardiac monitor shows “sinus tachycardia” (the prehospital ECG is unavailable).
During transport paramedics witness tonic-clonic seizure activity and 2 mg of IV lorazepam is given.
On arrival in the Emergency Department the airway is intact, respirations are shallow, and there is no response to painful stimuli. A nasopharyngeal airway is placed, the patient is ventilated with a bag valve mask, and then intubated via rapid sequence induction.
A 12-lead ECG is acquired.
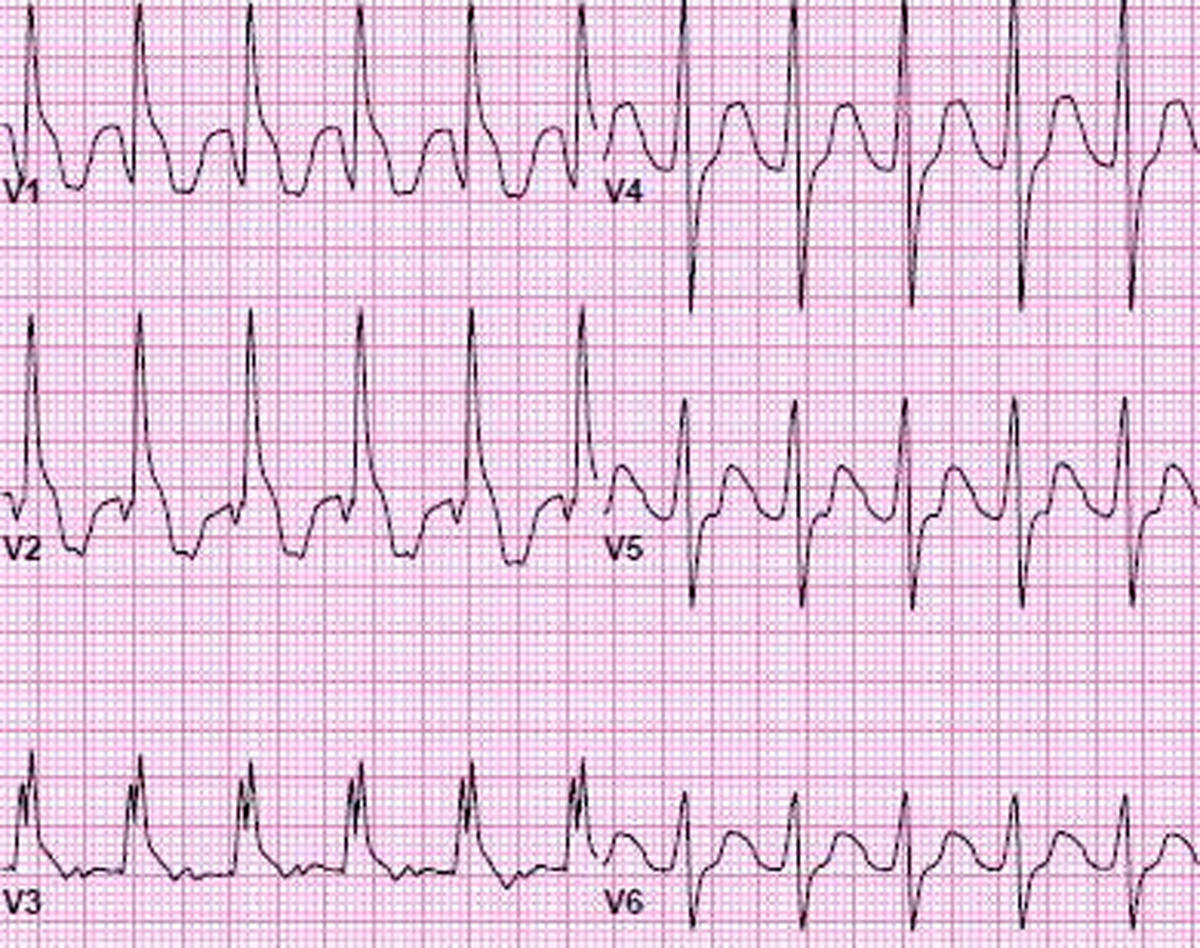
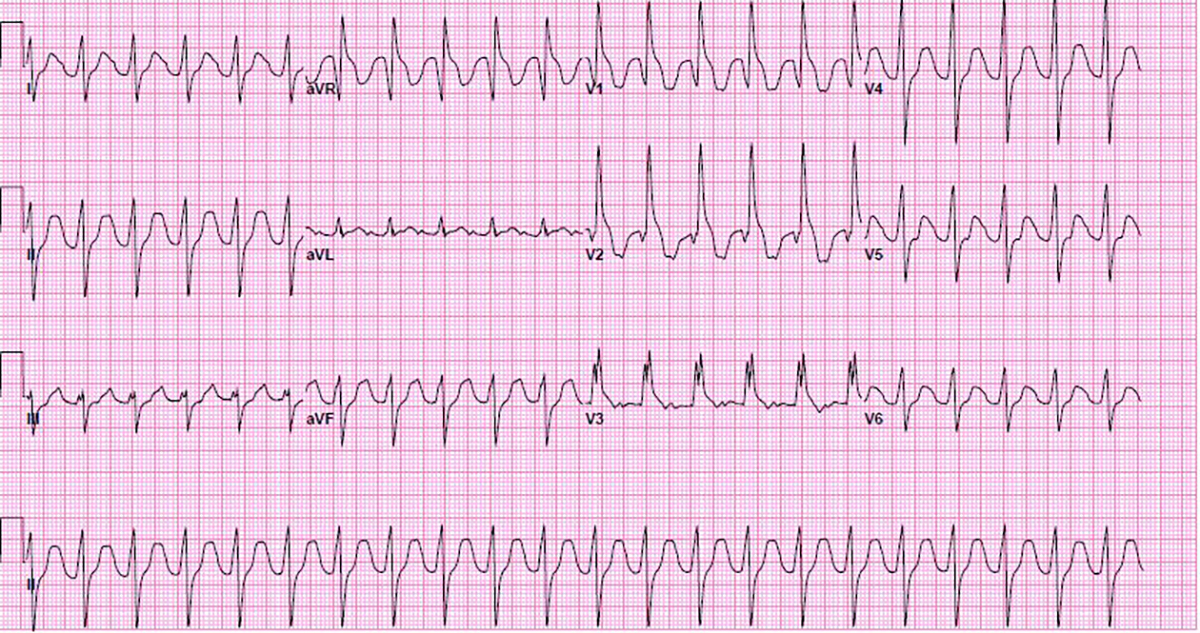
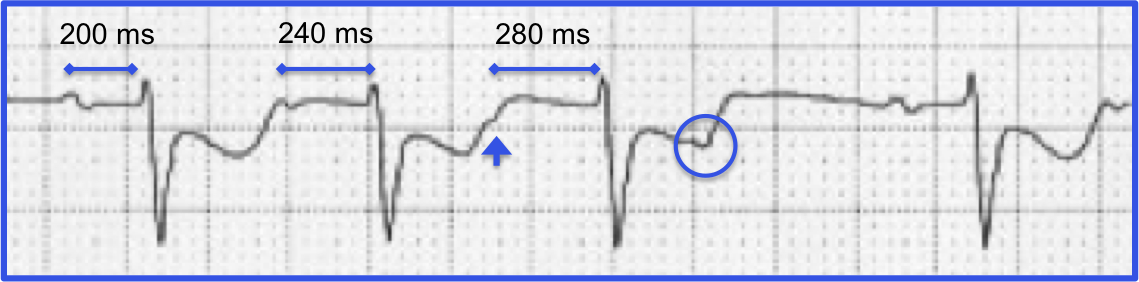
The QRS is wide at 138 ms. The QTc is prolonged at 596 ms. P waves can be seen in leads aVL and V3. This is most likely sinus tachycardia with toxicologic widening of the QRS.
200 mEq sodium bicarb is given and another 12-lead ECG is obtained.
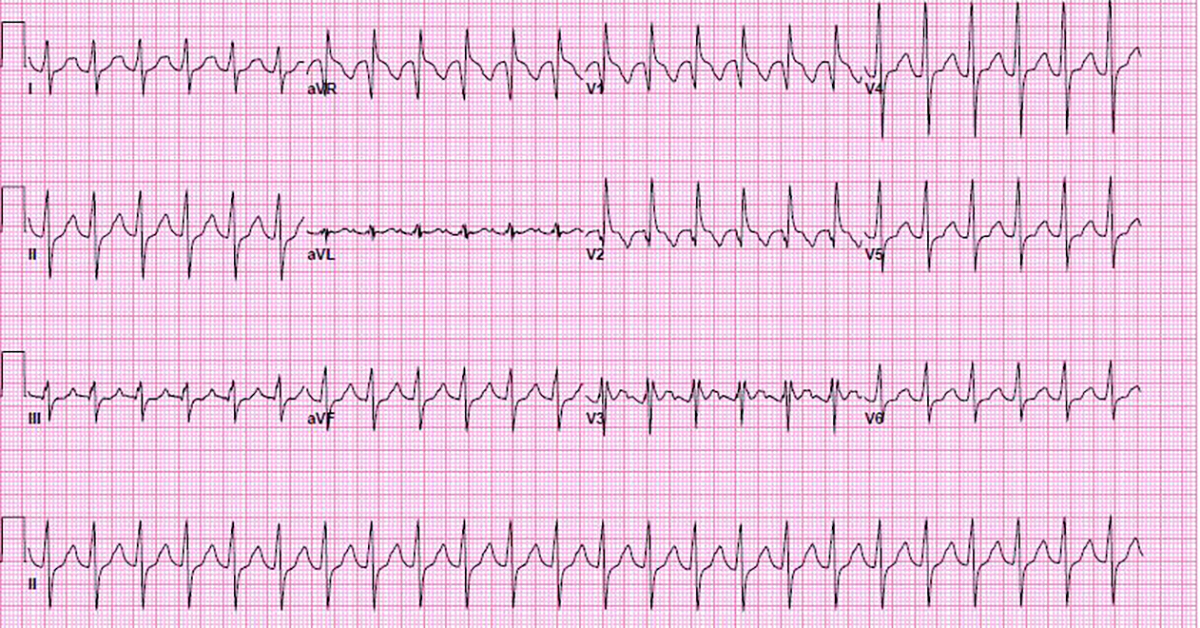
The QRS is now 130 ms and the QTc is 587ms.
An additional 200 mEq of sodium bicarb is given and the patient is started on a sodium bicarb drip, 150 mEq in 1,000 mL at 150 mL/hr.
30 minutes later the 12-lead ECG is repeated.
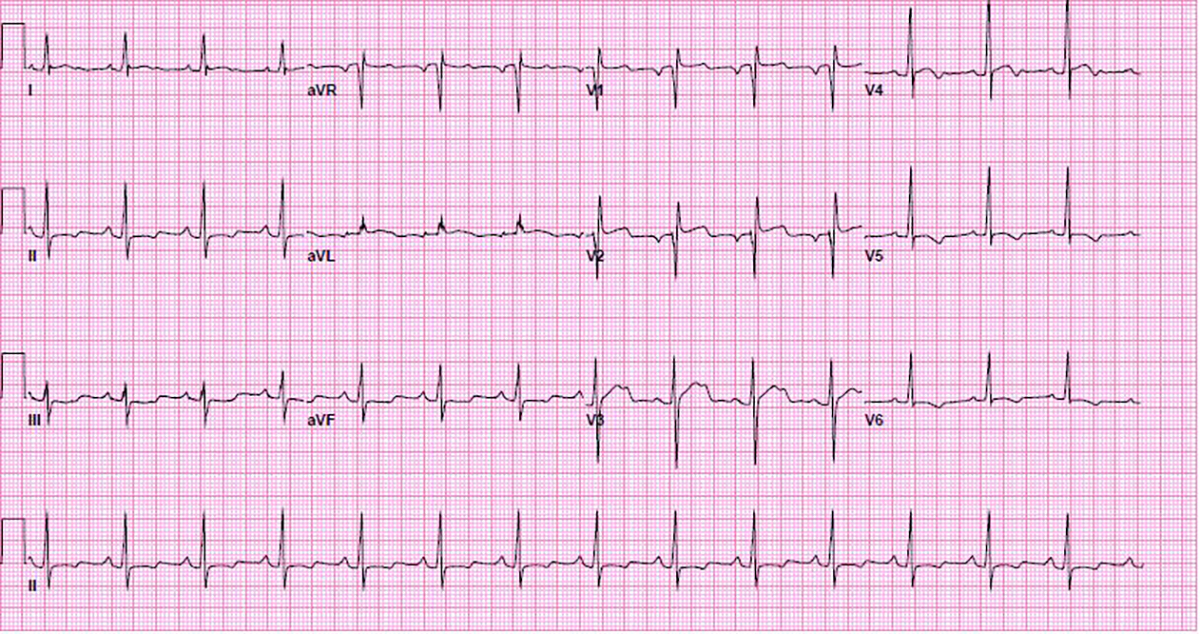
The QRS is now 90 msec with QTc 464 msec.
Now the QRS shows a normal duration but there are some troubling ECG findings.
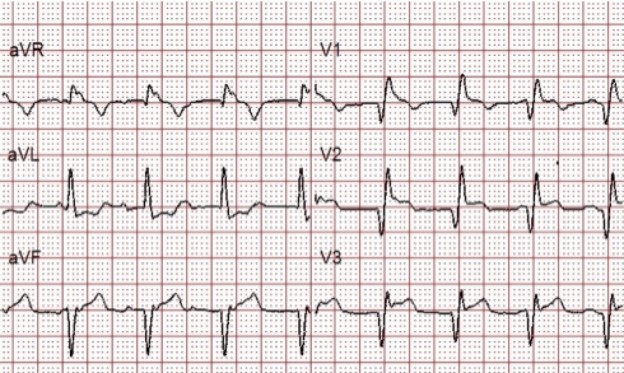
ST-segment elevation is noted in the right precordial leads (V1-V3) and the high lateral leads (I and aVL), with ST-segment depression in the inferior leads (II, III, and aVF). There are Q-waves in leads V1 and V2 with a QR pattern.
This was thought to be secondary to patient’s cocaine use and not from thrombotic disease so the cardiac cath lab was not immediately activated. Cardiac biomarkers remained negative, and the ST-segments normalized during hospitalization.
Discussion
Cocaine acts like a Class I antiarrhythmic which causes sodium channel blockade and widening of the QRS complex.
Treatment of toxicologic widening of the QRS consists of sodium bicarbonate (the sodium helps to overcome the blockade caused by the cocaine).
If QRS does not improve with sodium bicarbonate an alternative diagnosis other than toxicologic widening of the QRS should be considered.
Cocaine can also cause QT prolongation via blockade of the K+ rectifier channels.
Other cardiovascular events such as coronary artery spasm, myocardial infarction, hemorrhagic stroke, and aortic dissection related to sympathomimetic properties of cocaine should be considered in the differential diagnosis.
EMS was dispatched to a 48-year-old female having a seizure.
As they walked into the residence the patient was laying on the couch, not responding to commands. Her carotid pulse was palpable but the radial was absent. She was noted to be cyanotic and breath sounds were clear.
Side stream ETCO2 was placed under a non-rebreather (12 mm Hg) and rapid crystalloid infusion was initiated via an 18G IV.
A 12 Lead was obtained as another first responder went to retrieve the stretcher:
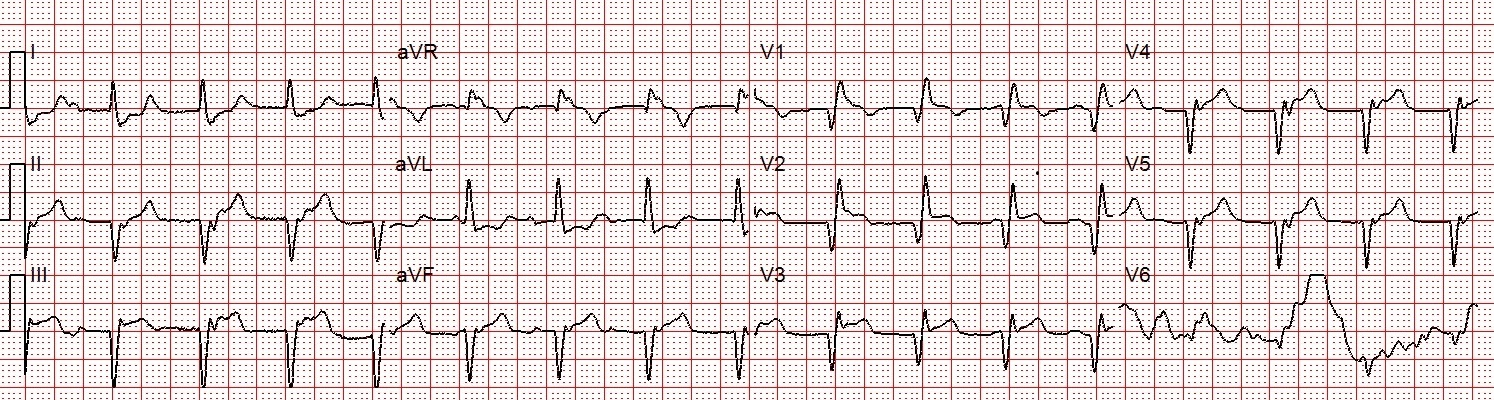
The QRS is wide (160ms) with RBBB morphology (QR in V1). Q-waves and ST-segment elevation are noted in the inferior and anterior leads.
Is this patient having a STEMI?
While the patient was being treated and extricated, a history was obtained from the husband. She had previously been on anticoagulation for a deep venous thrombosis that occurred secondary to hormone therapy. Combining the patient’s history with clinical findings, acute pulmonary embolism was suspected.
Clinical Evaluation of Suspected Pulmonary Embolism
The mortality rate for pulmonary embolism is 10% when diagnosed, but less than 50% are diagnosed at presentation. While there are many signs and symptoms of acute PE, 30% will have no perception of pain, but 90% will admit to a sensation of dyspnea.
Hypoxia with clear lungs is pulmonary embolism until proven otherwise
STEMI only causes hypoxia by causing pulmonary edema
Massive pulmonary embolism can result in a STEMI ECG, identical to ACS STEMI
Low end tidal CO2 is typical of massive PE. High end tidal CO2 is typical of severe pulmonary edema.
Using the ECG to Diagnose a Pulmonary Embolism
The ECG cannot “make the diagnosis” of PE, but can certainly be used to bolster the diagnosis and prompt further evaluation. Changes in the ST/T waves are normally seen in massive PE, and when present can help identify patients that are likely to deteriorate if immediate intervention is not performed. Had an appropriate history not been obtained in the case above, the ST-segment elevation could have been considered a coronary occlusion.
While many are familiar with the ECG finding known as “S1Q3T3” (S-wave in lead 1, Q-wave in lead III, and inverted T-wave in lead III), in a study comparing the incidence of various ECG findings in PE, Chan TC (2001) found that this finding is present only 11-50% of the time.
Sinus tachycardia is the most common ECG finding and is present 8-69% of the time, T-wave inversions in leads III and aVF are present 17-35% of the time, and T-wave inversions in leads V1 and V2 are present 27-68% of the time. Any time you see inferior or anterior T-wave inversions you should consider acute pulmonary embolism in your differential diagnosis.
This ECG is not a representative case of these changes but for a detailed explanation of ECG changes associated with PE you can review Dr. Ken Grauer’s ECG Blog #119.
Ischemia in Acute Pulmonary Embolism
Under normal physiological conditions, the right ventricle has very little resistance relative to the left ventricle. During acute, massive PE, there is increased right ventricular afterload that causes right ventricular dilation and an increasing workload that leads to severe demand ischemia of the right ventricle, which is already prone to ischemia because of the non-dominant blood supply.
It can be extremely difficult at times to distinguish between acute coronary occlusion and PE, which is why prehospital history can be invaluable. Flight Surgeon Dr. Samuel M Galvagno said:
“Indeed, in the management of PE, the prehospital provider’s history may provide the most important clue to the underlying disease process for patients who deteriorate before interrogation by emergency department staff”.
ETCO2 in Acute Pulmonary Embolism
When a blood clot occludes a pulmonary artery the lack of blood flow to the alveoli causes an increase in dead space ventilation. Areas of the lungs that once participated in gas exchange can no longer do so. Clinically, the SpO2 will remain low or not reflective of the amount of oxygenation. As dead space increases, ETCO2 decreases.
Case Conclusion
Immediately before transport the patient became extremely bradycardic and with agonal respirations. She was promptly intubated and given 1 mg of Atropine. The heart rate significantly improved but she remained in profound shock and cyanotic despite maximal oxygen therapy.
During transport she lost a pulse and had an asystolic arrest. Transport time to the ER was approximately 1.5-2 minutes, so chest compressions were started and the receiving facility was notified of the probable massive pulmonary embolism and cardiac arrest.
The receiving physician agreed that PE was the likely diagnosis. It just so happened that an interventionalist was in the ER and was pulled over to assist in the resuscitation. ROSC was achieved and an echo was performed showing acute right heart strain.
The patient was transported to the operating theater. Direct intra-arterial tPA was administered and clot extraction was attempted. The patient rearrested and further attempts at resuscitation was unsuccessful.
References
1.) Brady, William, and Jonathon Dean Truwit. Critical Decisions In Emergency And Acute Care Electrocardiography. Chichester, West Sussex: Wiley-Blackwell, 2009. Print.
2.) EMCrit, About, Josh Farkas, and the Crew. “Two EKG Patterns Of Pulmonary Embolism Which Mimic MI”. EMCrit. N.p., 2014. Web. 31 Dec. 2015.
3.) Galvagno, Samuel M. Emergency Pathophysiology. Jackson, Wyo.: Teton NewMedia, 2003. Print.
4.) Hqmeded-ecg.blogspot.com,. “Dr. Smith’s ECG Blog: Sudden Severe SOB And ST Segment Elevation: What Is The Diagnosis And Treatment?”. N.p., 2015. Web. 31 Dec. 2015.
5.) Marx, John A et al. Rosen’s Emergency Medicine. Philadelphia: Mosby/Elsevier, 2010. Print.
EMS (with physician on board) is dispatched to a 42-year-old male with a chief complaint of chest pain and “possible heart attack.”
The patient is found lying on the couch. He appears to be reasonably comfortable and indicates that “the pain has eased a bit” since EMS was contacted.
While the patient is being undressed and the monitoring leads are attached a quick and focused history is obtained using the “SOCRATES” mnemonic.
Site: Retrosternal
Onset: The pain started about 1 hour ago while folk dancing at a party and become progressively worse over about 10 minutes
Character: Poorly localized “tightness” or “discomfort”
Radiation: Both arms and back
Alleviating factors: Nothing makes the pain feel better
Timing: The pain is persistent and follows no pattern
Exacerbating: The pain seemed worse while walking to his car
Severity: 8/10
The patient is diaphoretic but it is not clear whether it is from dancing or related specifically to the chest discomfort. He denies nausea, vomiting, palpitations, or shortness of breath, and states that he has not collapsed.
Social history: Smoking (40 pack years) and liberal alcohol use
Medical history: Hypertension
Medications: Unknown antihypertensive
Allergies: NKDA
Vital signs:
RR: 16
HR: 84
NIBP: 125/82
Temp:
SpO2: 98% on room air
Physical exam:
The patient is a slightly overweight, stocky male, in no apparent distress. Mentation and speech are normal. Respirations appear normal. Breath sounds are clear bilaterally. Abdomen is soft and non-tender. No JVD or pitting edema. Strong radial pulses are noted bilaterally.
With this focused history and physical, acute coronary syndrome (ACS) is highest on list of differential diagnosis, with pulmonary embolism (PE) and aortic dissection possible, but much lower on the list.
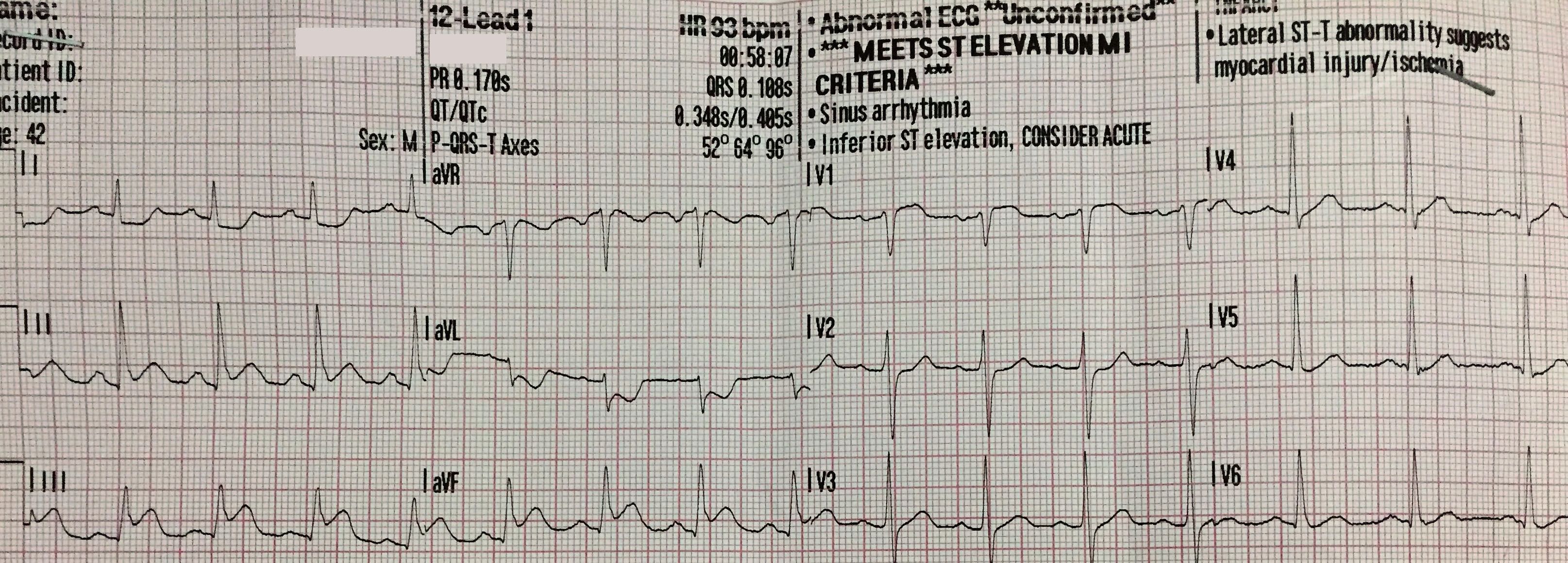
A 12-lead ECG is obtained.
ST-segment elevation is noted in leads II, III, and aVF with reciprocal changes in leads I and aVL. STE III > STE II suggests occlusion of the right coronary artery (RCA) which suggests the possibility of RV infarction. Of note, there is a small amount of ST-segment elevation in lead V1 (also suggestive of RV infarction).
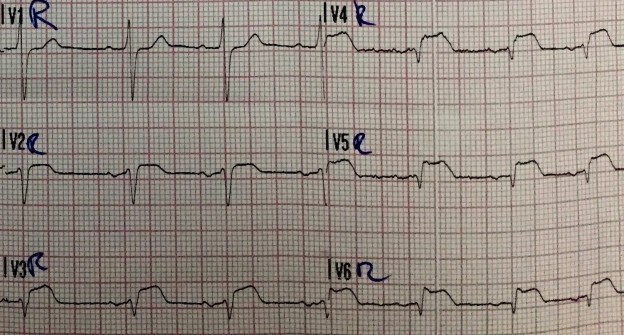
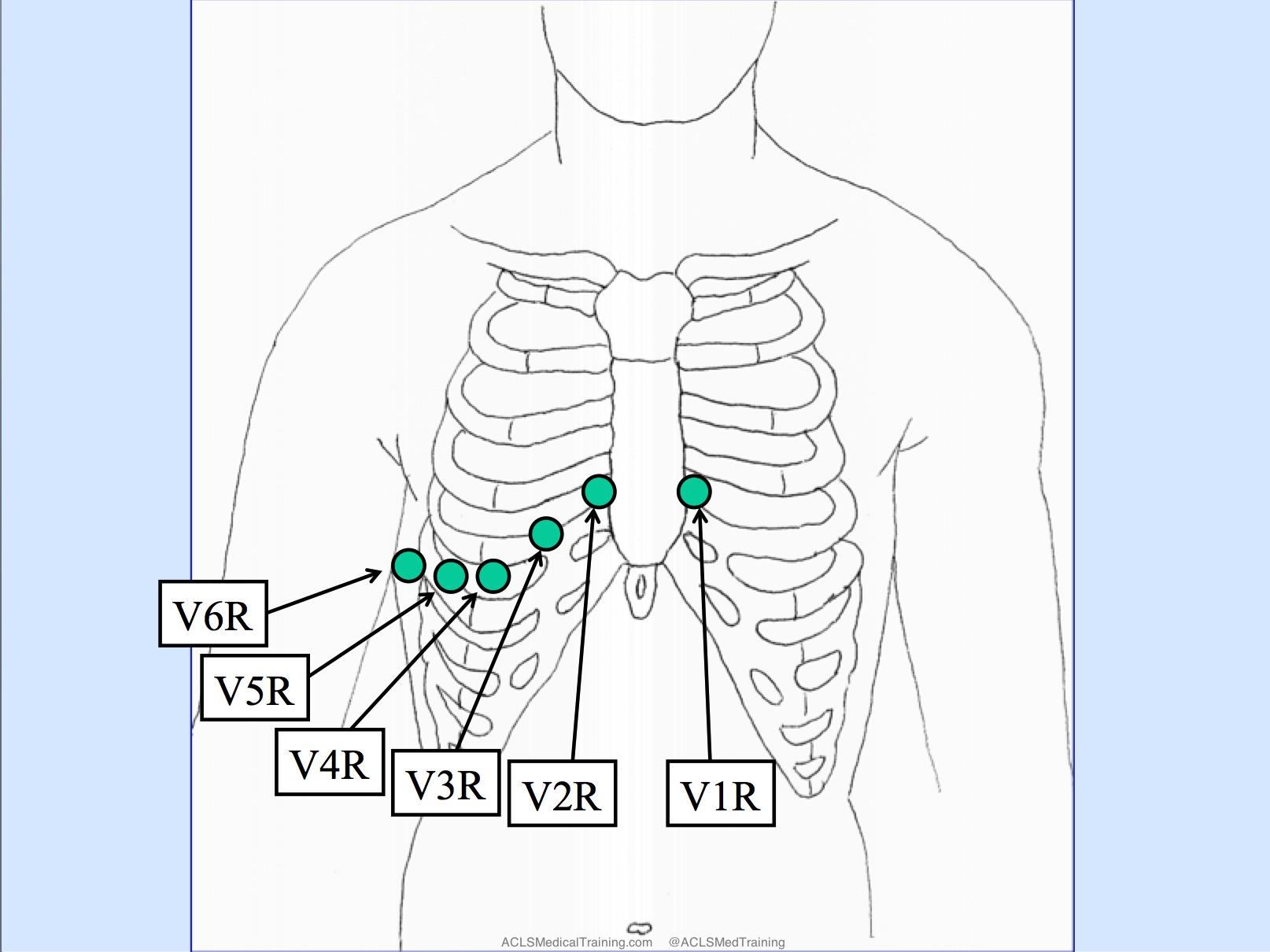
A right-sided 12-lead ECG is obtained. To accomplish this, the EMS crew places the precordial leads in the mirror-image position on the right side of the patient’s chest.
Editor’s note: Sometimes leads V1 and V2 are left in place and only leads V3-V6 are moved over to mirror image position on the patient’s right side.
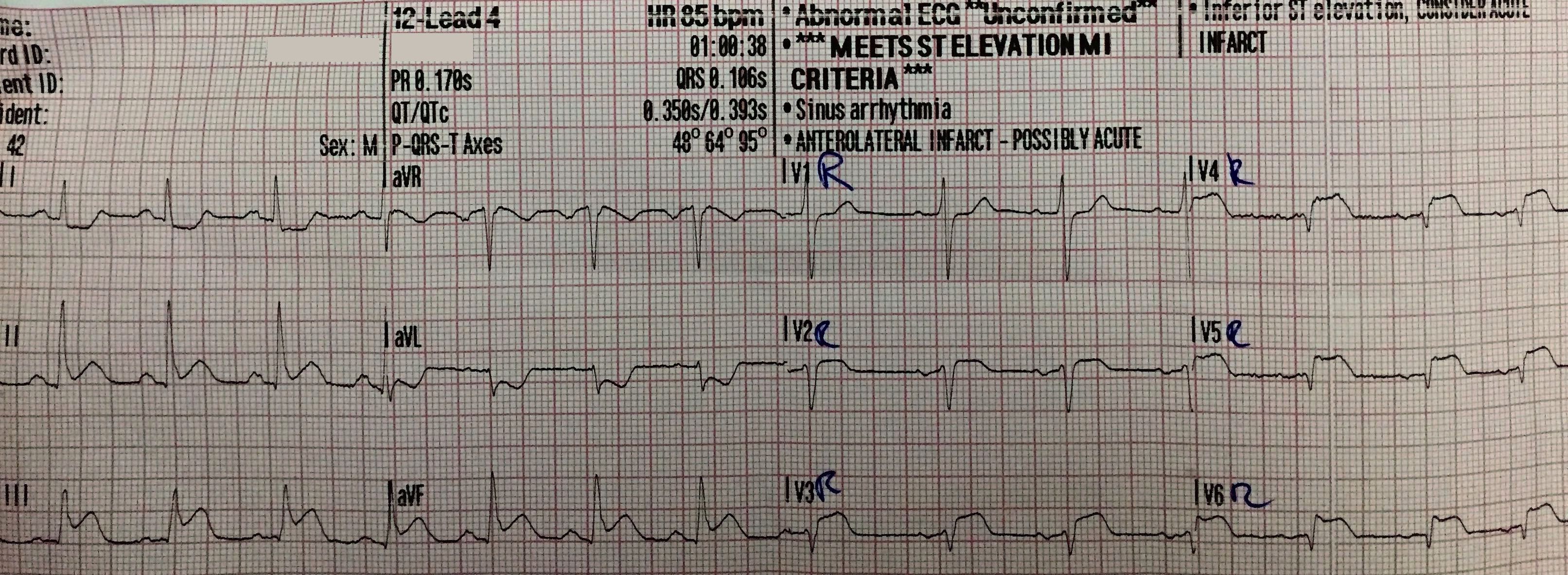
ST-segment elevation is noted in leads V2R, V3R, V4R, V5R, and V6R suggesting proximal occlusion of the RCA and right ventricular infarction.
Prehospital treatment:
Aspirin 250mg PO
Ringers lactate 500 ml
50 mcg of Fentanyl
Oxygen was not given as the patient reported and presented no signs of dyspnea
A trial dose (0.4 mg) NTG SL was given as RV infarction is a (relative) contraindication
The local receiving hospital and PCI unit are contacted by cell phone and the cardiac cath lab is activated.
Additional anticoagulant and antiplatelet therapy is given in the field.
Heparin 5000 units IV
Prasugrel 60 mg PO
The 15-minute ride to the PCI center is uneventful and patient’s symptoms improve.
The local ED team is notified of patient’s arrival and the transfer goes smoothly. The ED physician even exchanges a “high five” with the EMS crew.
As the prehospital physician is finishing his paperwork and discussing details of the case with the receiving physician, the nurses call for help. The team rushes into the resuscitation room to find the patient unresponsive with VF on the monitor.
CPR is initiated and the patient is defibrillated a total of 3 times. After the 3rd shock the patient erupts into wild seizure-like activity and lets out a scream followed by wild, deep inspirations.
The monitor shows a perfusing rhythm with a strong carotid pulse. The patient wakes up and asks, “What just happened?”
The patient is whisked away to the cardiac cath lab where a 95% occlusion to the RCA is successfully opened and stented. The patient is discharged a few days later.
Take-away points:
Know your differentials and obtain a swift, focused history (SOCRATES is a useful checklist)
All patients with chest pain should receive a 12-lead ECG early in the patient encounter
When the patient is suffering acute inferior STEMI a right-sided 12-lead ECG can help to identify right ventricular infarction
Be careful with nitroglycerin in the setting of right ventricular infarction
STEMI patients should be monitored continuously with defibrillation pads in place.
Don’t let your guard down! As Napoleon warned centuries ago, “The moment of greatest vulnerability is the instant immediately after victory.”
References:
1. https://en.wikipedia.org/wiki/SOCRATES_(pain_assessment)
2. Akbar A et al: Does this patient have an AMI? JAMA 1998;280(14):1256-63
3. Morris F, Brady WJ. ABC of clinical electrocardiography: Acute myocardial infarction-Part I. BMJ. 2002; 324: 831-4
4. http://emcrit.org/podcasts/emcrit-book-club-on-combat-by-grossman
EMS was called to an office building for a 61-year-old male complaining of chest pain.
Just prior to EMS arrival the patient became nauseated and lightheaded. When they found him he was lying supine on the floor and appeared ashen.
Onset: 45 minutes ago following a meeting with an important client
Provoke: Nothing makes the pain better or worse
Quality: “Squeezing”
Radiate: The pain does not radiate to the arms, back, neck, or jaw
Severity: 10/10
Time: No previous episodes
He was alert and oriented to person, place, time, and event with a relatively calm demeanor.
Vital signs were assessed.
RR: 24 (mildly labored)
HR: 60 (weak radial pulses)
NIBP: 87/40
Temp: 98.4°F
SpO2: 95% on room air
Breath sounds were clear bilaterally.
His medical history was remarkable only for hypertension and high cholesterol. He was unable to recall the names of his medications.
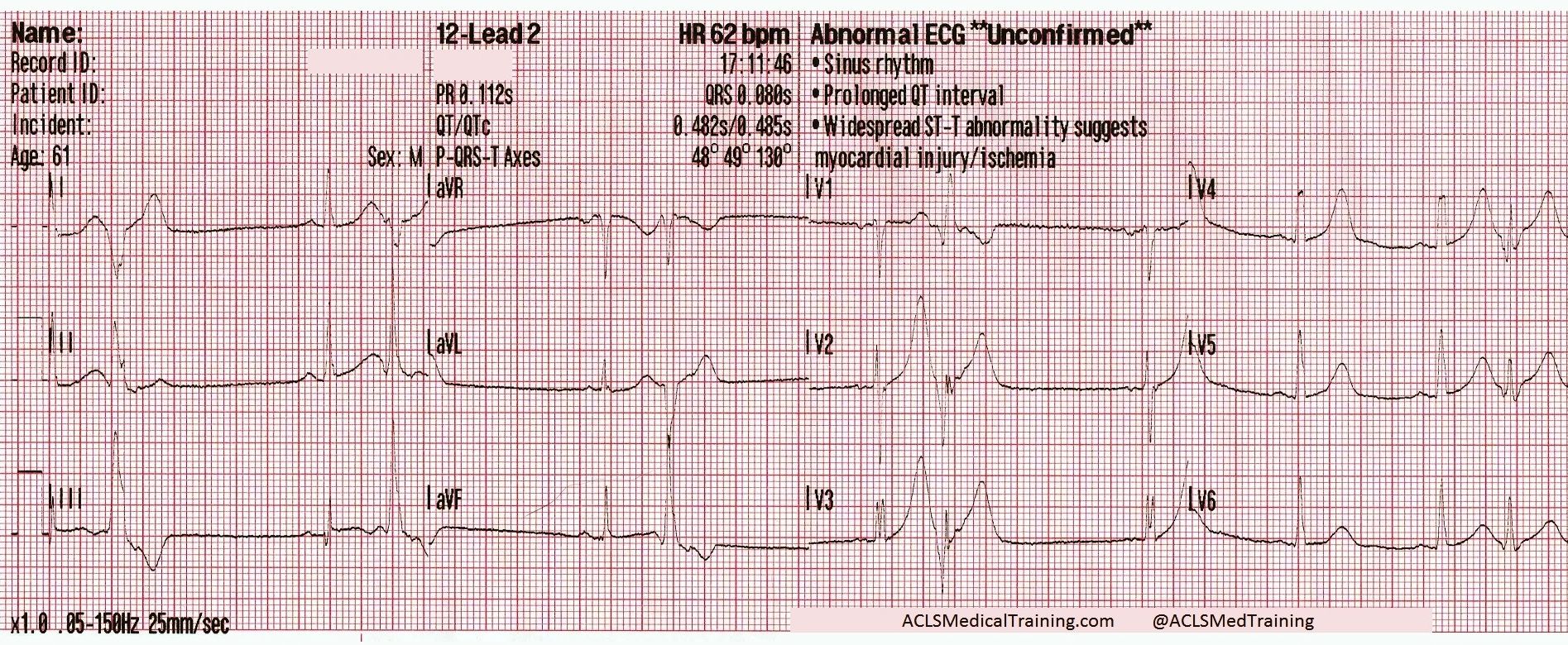
A 12-lead ECG was acquired.
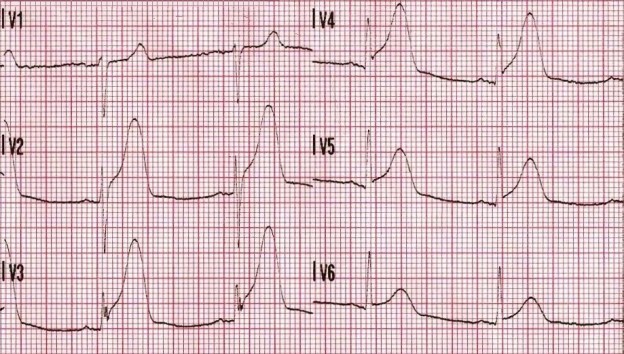
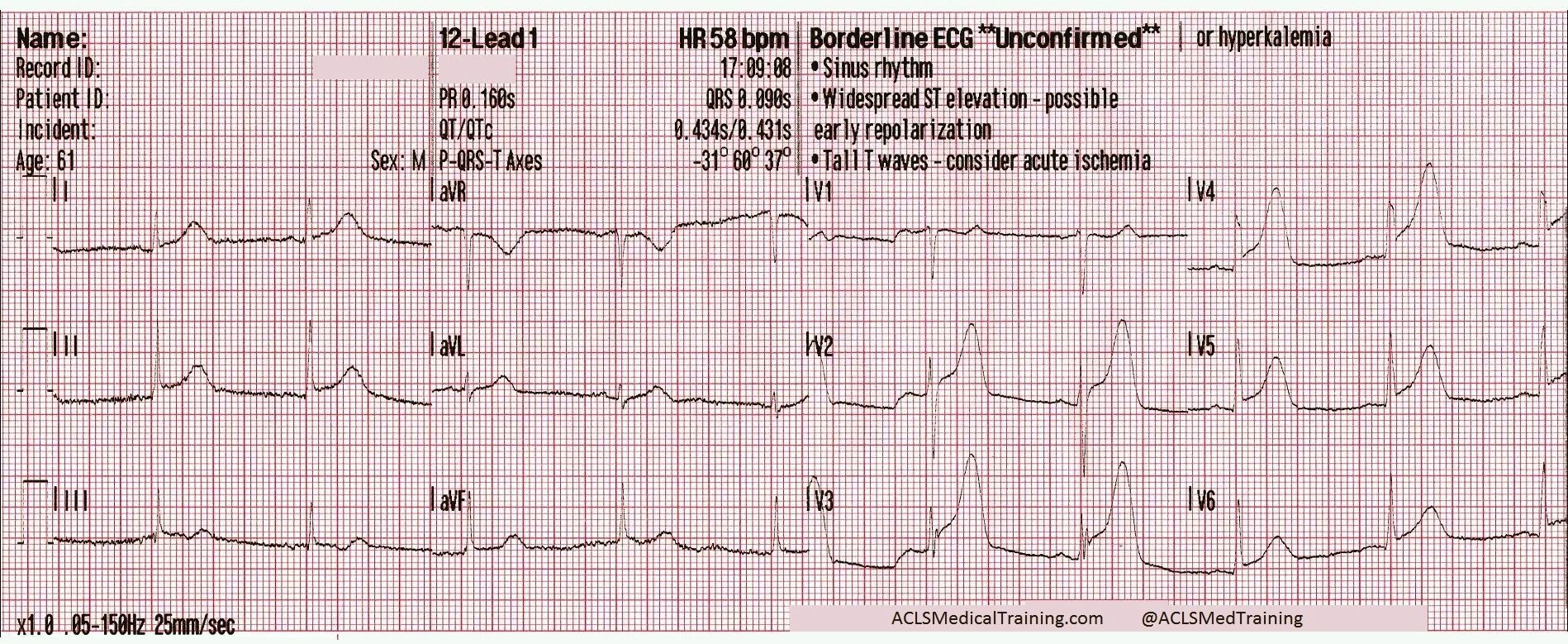
ST-segment elevation is present in leads V2-V5 and the T-waves are hyperacute. It is unclear why the computer is not giving the *** MEETS ST ELEVATION MI CRITERIA *** message. This does not look like early repolarization or hyperkalemia.
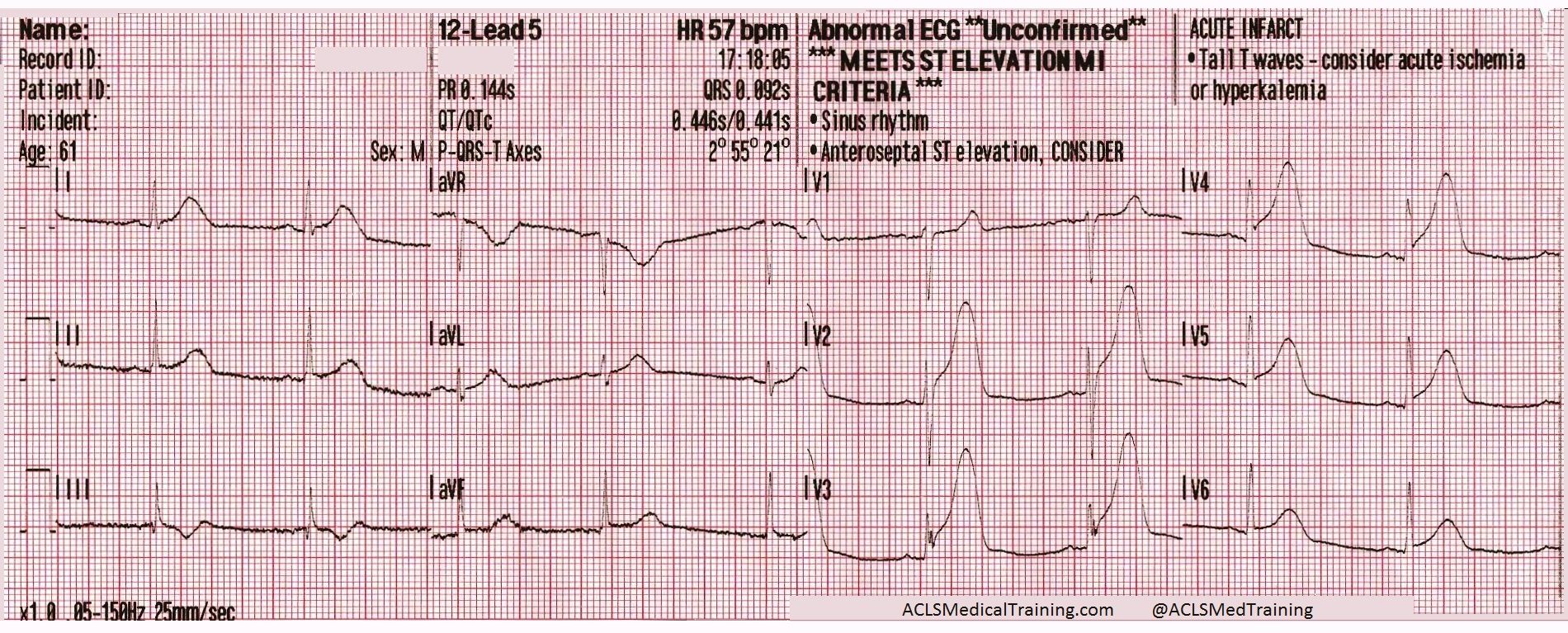
Then about two and a half minutes later…
We now have R-on-T PVCs, almost in bigeminy. The ST-segment elevation has resolved but the T-waves are still disproportionately large compared to the QRS complexes.
The treating paramedic correctly suspected that the patient was suffering an acute coronary syndrome, but there was uncertainty about whether or not it was a STEMI.
The patient was treated with aspirin and IV fluids for hypotension. The closest hospital was bypassed and the patient was transported to a PCI-hospital about 25 minutes away.
About 7 minutes later the patient’s blood pressure had improved to 102/69 but he was still complaining of 10/10 chest pain.
The ST-segment elevation has returned and the T-waves are unambiguously hyperacute. The computerized interpretive statement now reads *** MEETS ST ELEVATION MI CRITERIA ***
The ECG was transmitted to the hospital, IV fluids were continued, and 0.4 mg sublingual nitroglycerin was administered q 5min PRN, with moderate alleviation of the patient’s chest pain.
Vital signs were re-assessed.
RR: 20
HR: 64
NIBP: 114/76
SpO2: 98% on room air
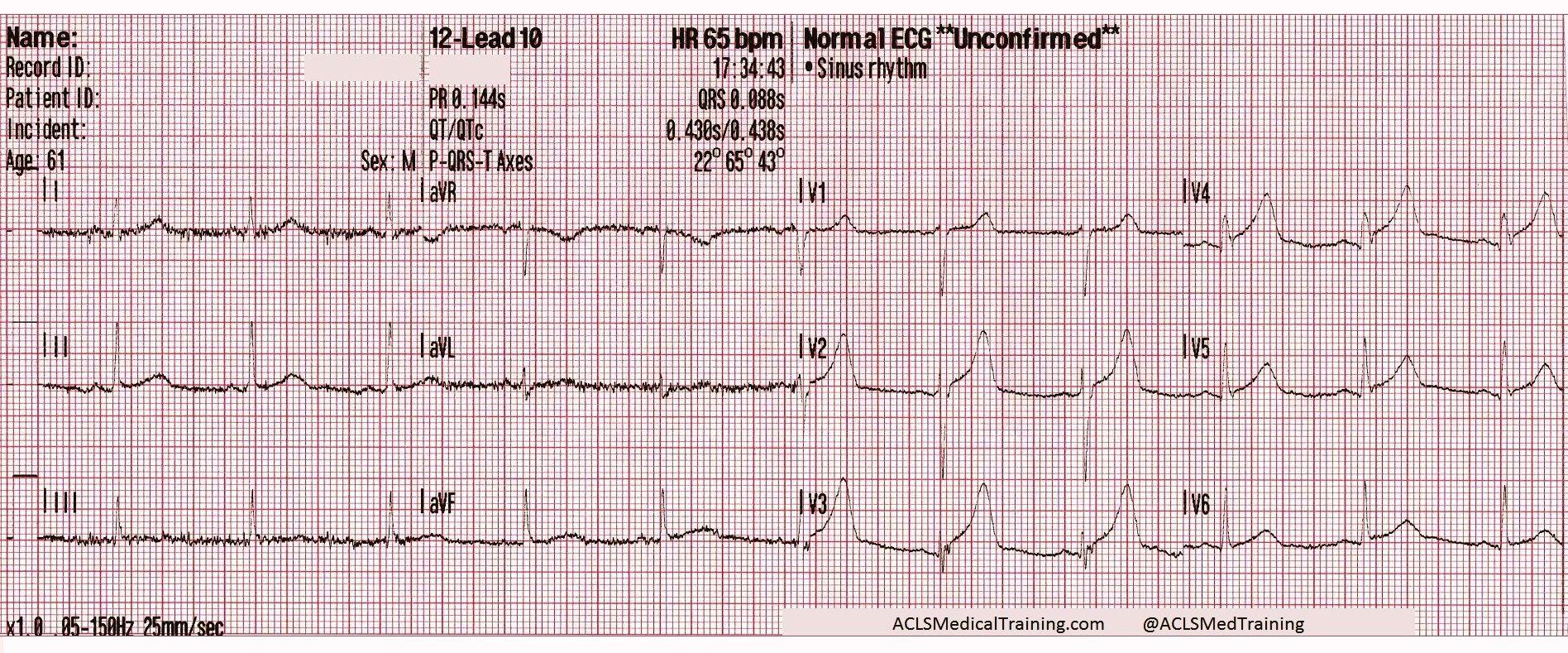
About fifteen minutes later this 12-lead ECG was acquired.
Once again the ST-segment elevation has resolved but there are still some troubling findings. R-wave progression has been obliterated and the T-waves are still disproportionately large when compared to the QRS complexes.
The ECG continued to show dynamic ST-segment and T-wave changes but they were mostly resolved by arrival at the hospital. The attending physician was waiting and there was some hesitation about sending the patient straight to the cardiac cath lab.
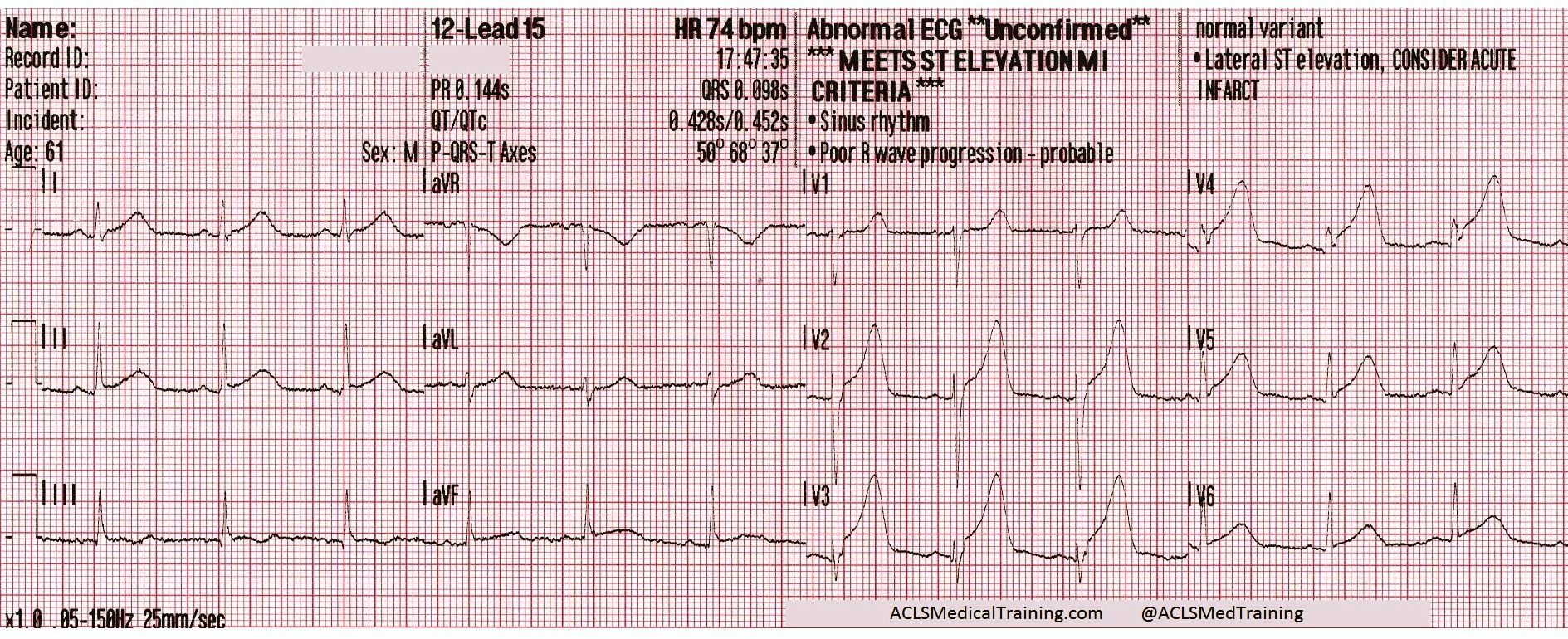
Before the patient could be moved from the paramedic’s stretcher the cardiac monitor automatically printed another 12-lead ECG.
The ST-segments and T-waves are back “on the way up” and once again the computer is giving the *** MEETS ST ELEVATION MI CRITERIA *** statement.
The cardiac cath lab was activated. Angiography revealed a 99% occlusion of the proximal left anterior descending artery (LAD), which was stented.
Discussion Points
1.) Obtain a 12-lead ECG with the first set of vital signs!
Myocardial infarction is a dynamic disease process. Coronary arteries can become totally occluded, partially reperfused, and totally occluded again!
There are case reports demonstrating resolution of ST-segment elevation after administration of nitroglycerin.1 Stephen Smith, M.D. (@SmithECGBlog) writes about it here. Tom Bouthillet (@tbouthillet) writes about it here. Brooks Walsh, M.D (@BrooksWalsh) writes about it here and questions whether it’s really due to nitroglycerin here.
2.) Should transient STEMI be sent directly to the cardiac cath lab?
The short answer is probably.
This hasn’t been widely studied but there is literature to support early activation of the cardiac cath lab when dealing with transient STEMI. One study published in Annals of Emergency Medicine concluded that positive serial ECGs were more sensitive and more specific for identifying ACS patients who require anti-ischemic therapy, evaluation for reperfusion, and/or admission to an ICU.2
Articles in Prehospital Emergency Care and American Heart Journal show that while patients with transient STEMI were likely to have less myocardial damage, higher rates of thrombolysis, and better cardiac function, they still benefit from early invasive therapy.3,4
Check out this post from Stephen Smith, M.D. for an example of what can go wrong if you don’t send them for PCI!
3.) What is the significance of hyperacute T-waves?
T-waves corresponding with myocardial injury become taller, wider, and more symmetrical in morphology — a phenomenon referred to as “hyperacute T-waves”.
Hyperacute T-waves are the most reliable indicator of salvageable myocardium at risk!
Hyperacute T-waves are considered to be a STEMI equivalent even when the conventional mm criteria are not met. Look for these changes both as the ST segments are “on the way up” and “on the way down.”
4.) What’s the significance of those PVCs?
Patients suffering an acute myocardial infarction are at increased risk of developing lethal arrhythmias. Ischemic myocardium is “irritable” and the presence of PVCs may be a helpful prognostic indicator.
Proximity of PVCs to the preceding T-waves (“R-on-T” PVCs) present a greater risk that the patient will develop VT or VF as premature depolarization occurs during the relative-refractory period of the previous cardiac cycle.
5.) What is the significance of bradycardia in LAD/LCX occlusion?
This patient was unable to provide the names for his antihypertensive medication so it’s likely that he was prescribed a beta blocker or calcium channel blocker.
A less likely possibility is that there was ischemia of the SA node brought about by repeated occlusion/reperfusion of the circumflex artery.
This has been found in case reports and animal studies to cause transient episodes of sinus bradycardia, even though sinus bradycardia is more typical of acute inferior STEMI (RCA occlusion). 5,6
References 1) Mahoney BD, Hildebrandt DA, Allegra P. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. Prehospital Emergency Care 2008;15:105, Abstract 24
2) Fesmire FM. Usefulness of Automated Serial 12-Lead ECG Monitoring During the Initial Emergency Department Evaluation of Patients With Chest Pain. Ann Emerg Med 1998;31(1):3-11
3) Ownbey M. et al. Prevalence and interventional outcomes of patients with resolution of ST-segment elevation between prehospital and in-hospital ECG. Prehosp Emerg Care 18(2);174-9. Apr-Jun 2014
4) Meisel SR, et al. Transient ST-elevation myocardial infarction: clinical course with intense medical therapy and early invasive approach, and comparison with persistent ST-elevation myocardial infarction. Am Heart J 155(5):848
5) Lin, C.-F., & Cheng, S.-M. (2006). Symptomatic Bradycardia due to Total Occlusion of Left Circumflex Artery without Electrocardiographic Evidence of Myocardial Infarction at Initial Presentation. Texas Heart Institute Journal,33(3), 396–398.
6) William A. Alter, III, PH.D., Robert N. Hawkins, PH.D., and Delbert E. Evans. Etiology of the Negative Chronotropic Responses to Transient Coronary Artery Occlusion in the Anesthetized Rhesus Monkey. Circulation. 1978;57:756-762
This is a case from the “old days” when prehospital 12-lead ECGs were still a bit of a novelty. Many of the details have been lost to time but patient’s heart rhythms will be the focus of this review.
The patient was a young woman in her late 40s who presented with syncope while playing tennis. Syncope during exercise is troubling and suggests a possible cardiac cause, which is potentially life threatening.
EMS arrived on scene and obtained a detailed history. The woman admitted to some chest discomfort. Vital signs were assessed and the cardiac monitor was attached.
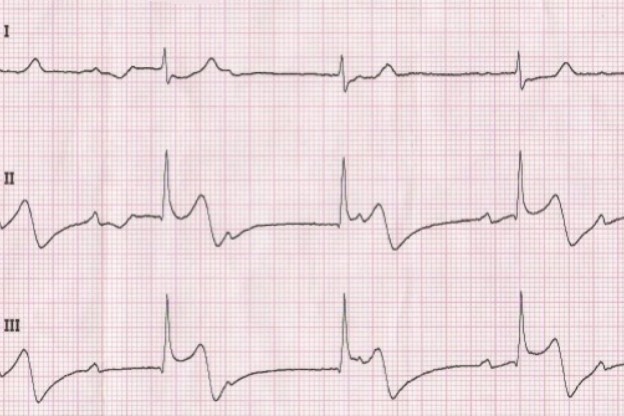
The initial ECG showed second degree AV block with 2:1 conduction.
This is often called second degree AV block type 2 with 2:1 conduction but second degree AV block with 2:1 conduction is untypeable.
There appears to be an acute injury pattern even though the rhythm strip is recorded in ‘monitor’ mode with the low frequency / high pass filter set to 1.0 Hz.
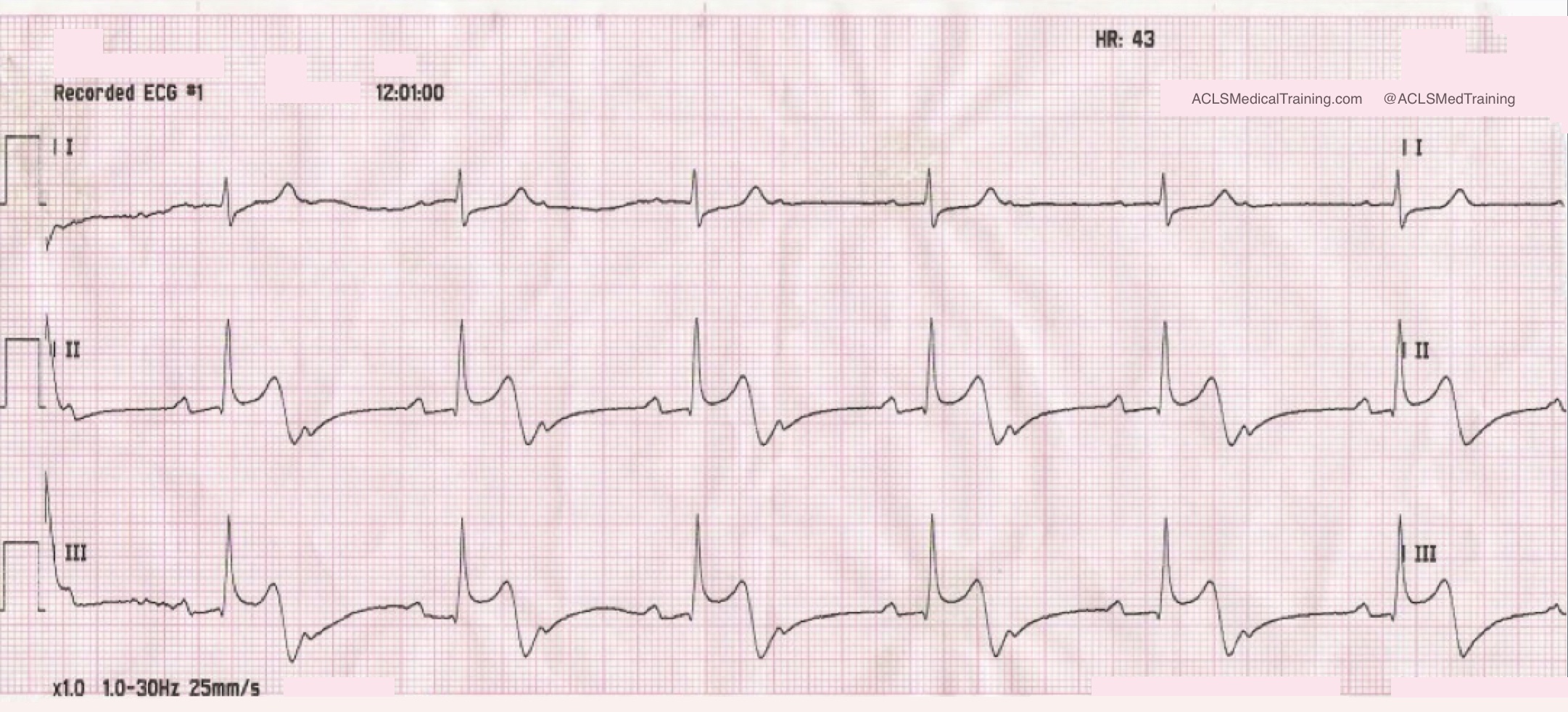
A few minutes later a rhythm change was noted on the monitor.
Now the rhythm is third degree AV block with junctional escape rhythm. The atrial rate is about 60 and the ventricular rate is 41.
(The initial 12-lead ECG showed poor data quality but paramedics understood that the patient was suffering acute STEMI.)
Aspirin was given and an IV was started. Nitroglycerin was also given and the patient became hypotensive.
Remember, this case is over 10 years old. At that time there was a lot less emphasis on things like right ventricular infarction and the cardiac cath lab was not activated based on the prehospital 12-lead ECG.
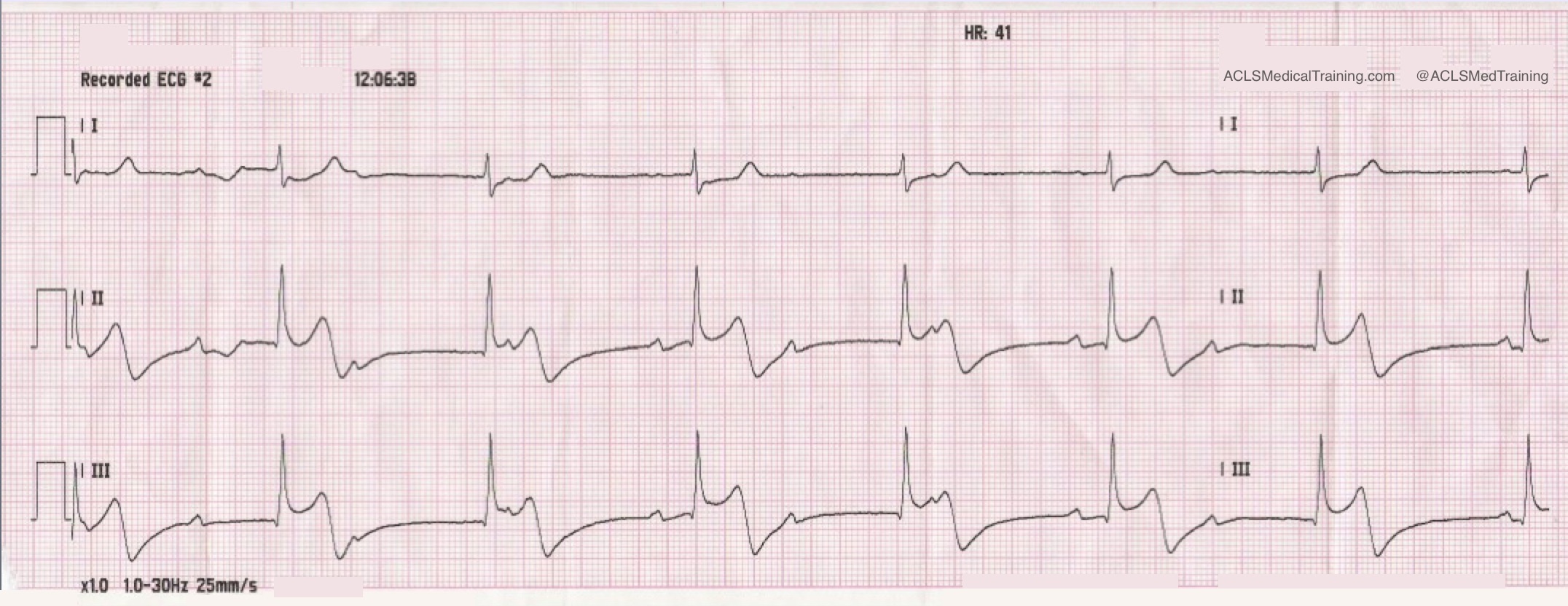
0.5 mg atropine was given rapid IVP and another 12-lead ECG was obtained.
The atrial rate has doubled to about 125. The ventricular rate has increased modestly to about 47. The ECG is diagnostic for acute inferior-posterior STEMI.
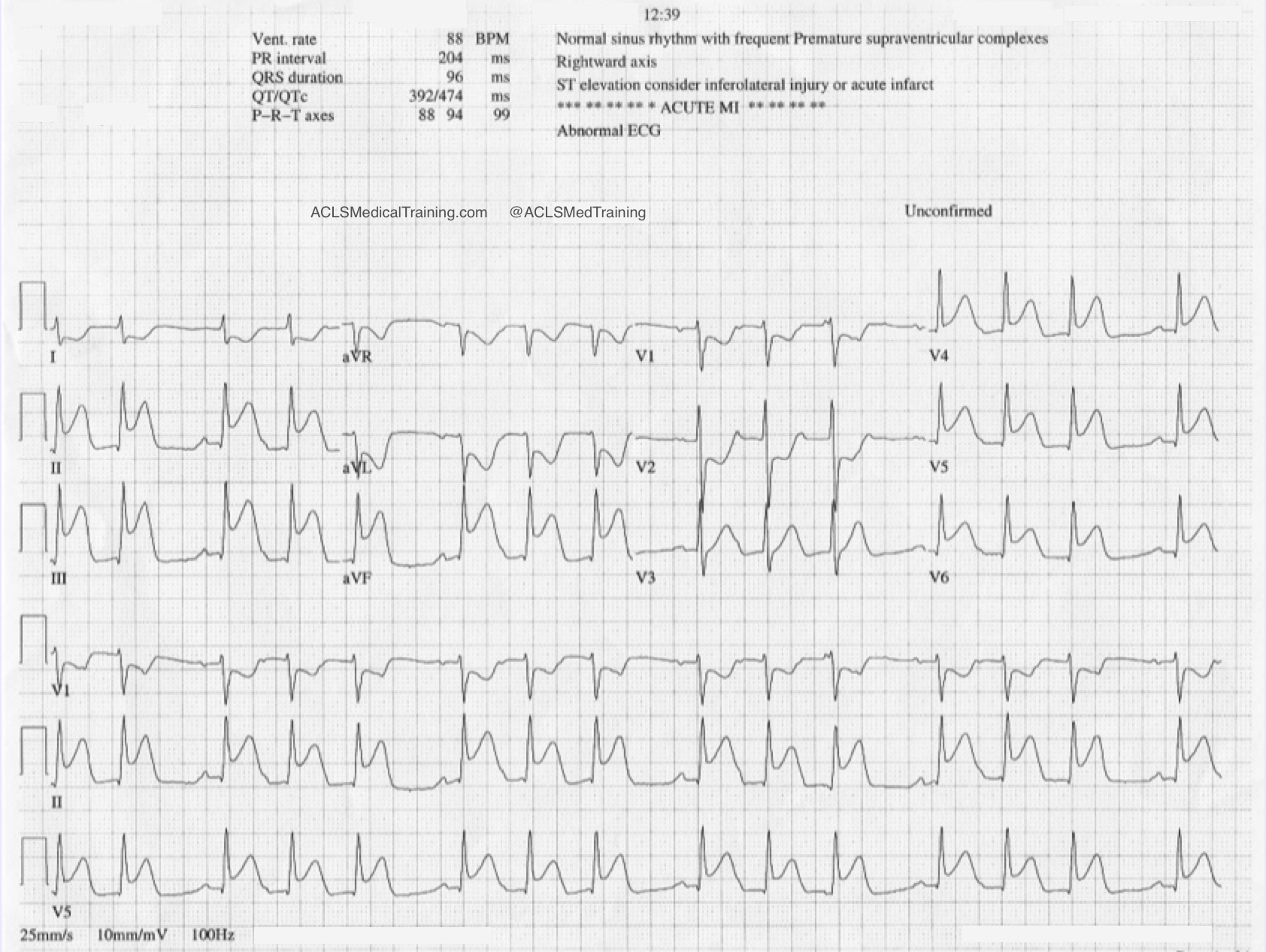
On arrival in the Emergency Department the staff obtained their own 12-lead ECG.
Now the heart rhythm is second degree AV block type 1 (Wenckebach).
How can you tell? In the first place we see clustering of QRS complexes (huge tip-off) and we already know that AV conduction is precarious. The initial cardiac cycle of each cluster shows a constant PR-interval.
When we take a closer look at the rhythm strip we see progressive prolongation of the PR-interval until a P-wave is “dropped” proving that the heart rhythm is second degree AV block type 1 (Wenckebach).
The ECG shows worsening of the ST-segment elevation. The patient was sent to the cardiac cath lab. As far as I know she made a full recovery.
Discussion
Heart blocks in the setting of acute STEMI can result either from ischemia of the AV node or increased parasympathetic tone, which is a manifestation of the Bezold-Jarisch reflex.
Consider these excerpts from Braunwald’s Heart Disease (Fifth Edition). It’s an old book but it contains some interesting information.
“The AV conduction system has a dual blood supply, the AV branch of the RCA and the septal perforating branch from the LAD. Therefore, complete heart block can occur in patients with either anterior or inferior infarction. Complete heart block develops in 5 to 15% of all patients with AMI; the incidence may be even higher in patients with RV infarction. As with other forms of AV block, the prognosis depends on the anatomical location of the block in the conduction system and the size of the infarction.”
“Complete heart block in inferior infarction usually results from an intranodal or supranodal lesion and develops gradually, often progressing from first degree or type I second degree block. The escape rhythm is usually stable without asystole and often junctional, with a rate exceeding 40 beats/min and a narrow QRS complex in 70% of cases and a slower rate and wide QRS in the others […] The mortality may approach 15% unless RV infarction is present, in which case the mortality associated with complete AV block may be more than doubled.”
“[P]atients with inferior MI and AV block have larger infarcts and more depressed right ventricular and left ventricular function than do inferior infarcts with no AV block. As already noted, junctional escape rhythms with narrow QRS complexes occur commonly in this setting…”
“Only when complete heart block develops in less than 6 hours after the onset of symptoms is atropine likely to abolish the AV block or cause acceleration of the escape rhythm. In such cases the AV block is likely to be transient and related to increases in vagal tone rather than the more persistent block seen later in the course of MI, which generally requires cardiac pacing.”